Narrow Palate Treatment in Frisco & The Colony, TX
Diagnosis & Correction by Dr. Baharvand & Dr. Kang — Palatal Expansion for Growing Patients, Arch Development for Adults, Plus Braces, Invisalign & Angel Aligners
📞 972.538.4343
Narrow palate correction at Elate Orthodontics — broadening the upper arch during growth, developing it strategically in adults
Narrow Palate — Frisco & The Colony, TX
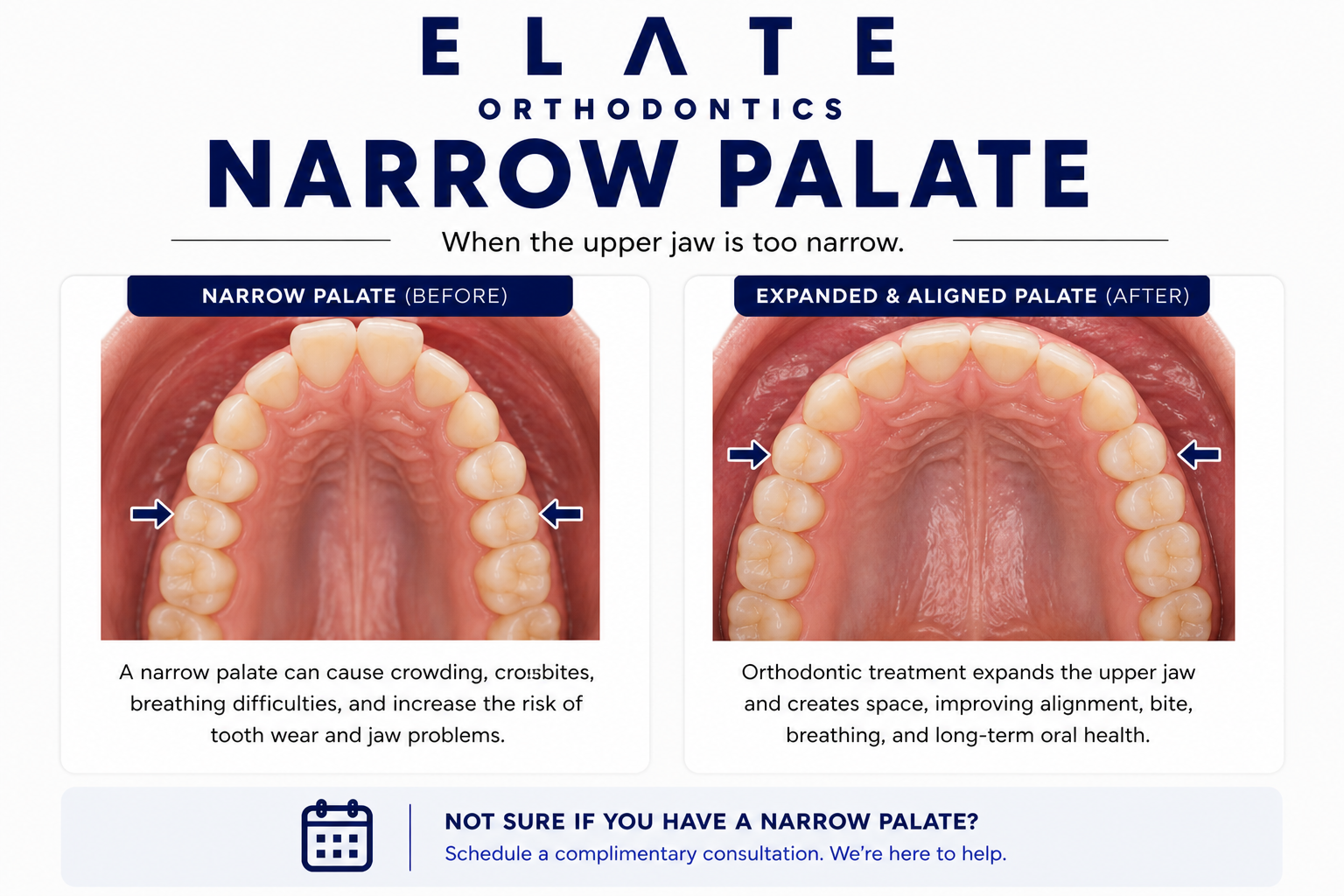
A Narrow Upper Jaw Sits at the Root of Crowding, Crossbite, and Often Airway Issues. Timing Determines What’s Possible.
A narrow palate refers to an upper jaw (the maxilla) that has not developed wide enough to comfortably accommodate the upper teeth or to fit properly with the lower jaw. The hallmark sign is a high arched palate — the roof of the mouth appears tall and pointed rather than gently curved. A narrow palate is rarely an isolated problem. It typically coexists with crowded upper teeth, posterior crossbite, mouth breathing, low tongue posture, and sometimes contributes to airway and sleep concerns. Identifying the narrow palate as the underlying structural issue often explains a constellation of seemingly separate problems in one patient.
At Elate Orthodontics, Dr. Kevin Baharvand and Dr. Julia Kang treat narrow palate cases in patients across Frisco, The Colony, Prosper, and Little Elm. Treatment options depend dramatically on age. In growing children and young adolescents, the upper jaw is two halves connected by a midpalatal suture that has not yet fused. A palatal expander can widen the upper jaw at this suture during the active growth window, producing true skeletal expansion. In adults, the suture has fused, so true skeletal expansion through routine appliances is no longer possible. Adult cases benefit from arch development — strategic broadening of the dental arch within the available bone — which improves alignment and function without trying to reopen a fused suture.
As an ABO board-certified practice with a published clinician on staff, our diagnostic approach reflects the depth of training that distinguishes specialty orthodontic care. We take comprehensive records at every consultation and explain exactly what we see using your own digital scans, panoramic X-rays, and clinical photos. For narrow palate cases, we explain honestly what is achievable at your specific age and design treatment that produces real, lasting results.
Recognizing a Narrow Palate
High Arched Palate
A high arched palate is the most recognizable sign of a narrow upper jaw. The roof of the mouth appears tall and pointed rather than gently curved. The palate may look almost vault-like in severe cases. This shape is partly genetic but is also strongly associated with mouth breathing during childhood, when the tongue does not rest against the palate to shape it during growth.
Parents often notice the high arched palate when their child is yawning or laughing. It is a strong indicator that an orthodontic evaluation is warranted, even when the smile itself looks fine.
Posterior Crossbite
Many narrow palate cases coexist with a posterior crossbite, where the upper back teeth bite inside the lower back teeth instead of outside them. This happens because the upper jaw is too narrow to fit normally over the lower jaw. Unilateral posterior crossbites often cause the lower jaw to shift to one side every time the patient bites, which can lead to facial asymmetry and midline shift over years of growth.
Treating the narrow palate with palatal expansion (in growing patients) often resolves the crossbite at the same time. This is one of the most common Phase 1 treatment scenarios.
Crowding & Cheek Indentations
A narrow palate often produces visible indentations on the inside of the cheeks where the cheek tissue presses inward against narrow upper teeth. The narrow arch also forces upper teeth to crowd, rotate, or block out (particularly canines). When a child has both a narrow palate and crowding, addressing the palate width first often creates space for the teeth to align without extractions later.
This is why we recommend evaluation at age 7 — catching narrow palate cases during the active growth window can dramatically simplify or even prevent the need for later orthodontic treatment with extractions.
Mouth Breathing & Sleep Concerns
A narrow palate is closely connected to airway function. The roof of the mouth and the floor of the nasal cavity are the same bone. A narrow, high palate often means a constricted nasal floor, contributing to chronic mouth breathing, snoring, and disrupted sleep in children. Children who consistently breathe through their mouth at night, snore, or wake unrefreshed often benefit from evaluation that includes assessment of palate width.
Our airway orthodontics page covers this connection in more depth. Addressing the narrow palate in growing patients often improves airway function alongside the orthodontic benefits.
Most narrow palate patients have a combination of these signs. Comprehensive diagnosis identifies which factors are contributing to the case and the right approach for the patient’s age.
Underlying Causes
What Causes a Narrow Palate?
Jaw size and palate shape are largely inherited. If one or both parents have a narrow palate or required orthodontic treatment for crossbite or crowding, their children are at higher likelihood of developing similar patterns. Family history is one of our routine screening questions for children at the age 7 evaluation.
When children consistently breathe through the mouth, the tongue rests low rather than against the roof of the mouth. The tongue is one of the strongest forces shaping the upper jaw during growth — without normal tongue pressure on the palate, the jaw often develops narrower than it should. Mouth breathing in children is a critical risk factor for narrow palate development.
Chronically enlarged tonsils or adenoids force children to breathe through their mouths, which then drives the low tongue posture and altered jaw growth that produces a narrow palate. Identifying and addressing tonsil and adenoid issues with an ENT specialist early — alongside orthodontic treatment — produces better outcomes than treating either in isolation.
Children with chronic environmental allergies or recurrent sinus issues often default to mouth breathing because nasal breathing is uncomfortable. Years of mouth breathing during growth produce the same downstream effect — low tongue posture, altered jaw development, and a narrow palate. Coordinating with allergists or ENT specialists is part of comprehensive care for these patients.
Prolonged thumb sucking or pacifier use past age 4 to 5 alters the resting position of the tongue and applies pressure that narrows the upper jaw. Habit-driven palate narrowing is one of the most common reasons we see this condition in young patients. Stopping the habit alone is not usually enough to reverse the structural change once it has developed.
A restrictive frenum under the tongue (tongue-tie) prevents the tongue from resting in its normal high position against the palate. Without that contact during years of growth, the upper jaw often develops narrow. Diagnosing tongue-tie is part of our evaluation for narrow palate cases, and we coordinate with appropriate specialists when release is needed.
Why a Narrow Palate Is More Than Cosmetic
A narrow palate is one of the underlying structural conditions that drives multiple downstream problems. Treating the palate width is often the most efficient way to address several of those problems at once. In growing children, palatal expansion can correct posterior crossbite, create space that prevents extractions later, eliminate functional shifts that would have caused facial asymmetry, and improve airway function — all from a single appliance worn for several months.
In adults, the structural narrow jaw is no longer correctable through routine non-surgical means, but its functional consequences (crowding, alignment problems, dental compensation) can be addressed effectively with arch development and comprehensive orthodontics. The honest conversation about what is and is not achievable in adulthood is part of what we do at consultation.
What an Untreated Narrow Palate Causes
Severe crowding of upper teeth, often requiring extractions in adolescence that could have been avoided
Posterior crossbite that worsens with growth and often produces functional shift of the lower jaw
Facial asymmetry developing over years of asymmetric chewing in unilateral crossbite cases
Impacted upper canines from insufficient arch space
Continued mouth breathing with downstream effects on facial development, dental health, and sleep
Snoring, restless sleep, and other airway concerns potentially associated with constricted nasal floor
Loss of the simple expansion window once the midpalatal suture fuses in late adolescence
Treatment Approach
How We Treat Narrow Palate at Every Age
Treatment for narrow palate is one of the most age-dependent decisions in orthodontics. The midpalatal suture — the seam where the two halves of the upper jaw meet — is open in childhood and progressively fuses through adolescence. The age at which this fusion completes varies but typically happens between ages 14 and 17 in girls and slightly later in boys. Once fused, true skeletal palatal expansion is no longer possible through routine orthodontic appliances. Our treatment approach reflects what is achievable at each stage.
Children (Ages 7–10) — The Prime Window
This is the prime treatment window for narrow palate. The midpalatal suture is wide open, palatal expansion produces predictable skeletal widening of the upper jaw, and the changes typically support good airway function and prevent crowding. Treatment is usually 6 to 9 months of expander wear followed by a retention period.
Phase 1 palatal expansion at this age often eliminates the need for later extractions and resolves coexisting posterior crossbite. The single most powerful intervention available for growing narrow palate cases.
Teens (Ages 11–14)
Through early adolescence, palatal expansion is still effective for most patients because the midpalatal suture has not yet fully fused. Expansion is typically combined with comprehensive orthodontic treatment using braces or aligners. The expansion phase remains predictable for most teens through age 13 to 14.
Late teens with completing fusion may benefit from comprehensive treatment with arch development rather than skeletal expansion. We assess fusion status and treatment options at consultation.
Adults — Arch Development Approach
In adults, the midpalatal suture has fused, so true skeletal expansion through routine appliances is not what we offer. We do not provide adult palatal expansion. Instead, we use arch development — strategic broadening of the dental arch within the available bone, combined with comprehensive orthodontic treatment using braces, Invisalign, or Angel Aligners. This addresses crowding, alignment, and bite issues without claiming to widen the underlying jawbone.
For adults with severe skeletal narrow palate where significant skeletal change is genuinely needed, surgical options exist that we can discuss honestly. We tell you what arch development can and cannot achieve in your specific case.
Treatment Options
Treatments We Use to Address Narrow Palate
Palatal Expander (Growing Patients)
The defining treatment for narrow palate in growing children and young adolescents. The expander widens the upper jaw at the midpalatal suture before it fuses, producing true skeletal expansion. Highly effective in patients ages 7 to 13. Often the first phase of treatment in cases that will later need comprehensive orthodontics in adolescence.
Arch Development (Adult & Late Teen Approach)
For adults and patients whose midpalatal suture has fused, arch development uses comprehensive orthodontic treatment to broaden the dental arch within the available bone. This improves crowding and alignment without claiming to widen the underlying jaw. Arch development is what we offer adults in place of skeletal expansion. We are direct about the difference and what each can achieve.
Traditional Braces
The most reliable platform for the comprehensive treatment that follows palatal expansion in growing patients, and for arch development in adults. Braces give us precise control over each tooth and remain the gold standard for the most demanding alignment cases that often accompany narrow palate.
Clear Braces
Same effective mechanics as traditional braces with tooth-colored brackets that blend with natural enamel. A great option for teens and adults treating narrow palate downstream effects who want the predictability of braces with less visibility during treatment.
Invisalign
Modern Invisalign protocols include arch development capabilities with precision attachments that broaden the dental arch effectively in adolescent and adult cases. For adults addressing the downstream effects of a narrow palate, Invisalign with arch development is often a strong option.
Angel Aligners
A clear aligner system we offer at Elate Orthodontics for appropriate cases. Like other clear aligner brands, Angel Aligners can support arch development for adolescent and adult cases addressing narrow palate downstream effects, with treatment plans tailored to each patient’s anatomy.
Pediatric Orthodontics (Phase 1)
For young children with narrow palate, Phase 1 interceptive treatment combines palatal expansion with habit appliances, space management, and ENT or myofunctional therapy coordination as needed. Comprehensive Phase 1 care addresses the narrow palate alongside its contributing factors.
ENT & Myofunctional Coordination
Many narrow palate cases involve mouth breathing driven by enlarged tonsils and adenoids, allergies, or tongue posture issues. We coordinate with ENT specialists for airway evaluation and with myofunctional therapists to retrain tongue posture during and after orthodontic treatment. Addressing the underlying factors produces more stable long-term results.
AAO Recommendation
Narrow Palate Has the Most Time-Sensitive Treatment Window in Orthodontics
The American Association of Orthodontists recommends an evaluation by age 7. For narrow palate, this matters more than for almost any other orthodontic condition because the treatment window is biologically time-limited. Once the midpalatal suture fuses in late adolescence, true skeletal palatal expansion through routine appliances is no longer possible. The same case caught at age 8 with palatal expansion may produce a fundamentally different outcome than the same case caught at age 22, where we can only address the downstream tooth-level issues through arch development.
Most children evaluated at age 7 do not need treatment immediately. The point is to identify children with narrow palate patterns and decide whether to start treatment soon, monitor closely, or revisit at a later age. We are honest about which cases truly need early intervention and which can wait. Adults with narrow palate downstream effects can still achieve excellent outcomes through arch development and comprehensive orthodontics, but we do not offer adult skeletal expansion and we explain that distinction directly.
See Real Outcomes
Narrow Palate Cases From Our Practice
Our before-and-after gallery includes real narrow palate corrections at Elate Orthodontics, ranging from Phase 1 expansion cases that resolved crossbite and prevented later extractions, to teen comprehensive cases combining expansion with full orthodontic treatment, to adult cases addressing the downstream effects of narrow palate through arch development. Each case shows the diagnosis, the appliances used, and the final result.
Common Questions
Narrow Palate FAQ
We do not provide adult palatal expansion at Elate Orthodontics. By the time the midpalatal suture has fused (typically completing in the late teens), true skeletal expansion through routine appliances is no longer possible. For adults, we use arch development — strategic broadening of the dental arch within the available bone — combined with comprehensive orthodontic treatment. This produces excellent outcomes for the alignment and crowding issues that result from narrow palate, even though we are not widening the underlying jaw bone itself.
Signs that warrant evaluation include a high arched palate visible when the child yawns or laughs, posterior crossbite (upper back teeth biting inside lower back teeth), severe upper tooth crowding, chronic mouth breathing or snoring, and family history of narrow palate or crossbite. The age 7 orthodontic evaluation is the right time to assess these signs and determine whether intervention is needed.
Palatal expansion in growing children is generally well-tolerated. Most patients report mild pressure or tightness for the first few hours after each adjustment, particularly during the early weeks of expansion. Children adapt to the appliance quickly and resume normal eating and speaking within a few days. The expansion process itself is gradual and not painful for most patients.
Palatal expansion produces subtle changes in the upper jaw that can sometimes be reflected in a slightly broader smile or improved facial balance. The changes are generally positive for facial esthetics. In children with very narrow palates and dental crowding, expansion sometimes resolves a constricted appearance to the smile that parents had not consciously noticed before treatment.
Phase 1 palatal expansion in growing children typically takes 6 to 9 months of active expansion, followed by a retention period to allow new bone to form in the widened suture. Comprehensive treatment in adolescence following expansion typically takes 18 to 24 months. Adult arch development through comprehensive orthodontics typically takes 18 to 24 months depending on case complexity.
Most PPO dental insurance plans include orthodontic benefits that apply to narrow palate treatment, particularly Phase 1 expansion in growing children. Coverage often includes both the expander appliance and any subsequent comprehensive treatment. Coverage varies by plan. We are in-network with most major PPO carriers and offer flexible financing through Cherry to make treatment accessible regardless of insurance coverage.
Why Frisco & The Colony Patients Choose Elate Orthodontics for Narrow Palate
Narrow palate is one of the conditions where the difference between honest assessment and overpromising matters most. We are direct about what is achievable at each age and what is not. For children, palatal expansion produces real skeletal change during the active growth window. For adults, arch development addresses the downstream tooth-level effects but does not widen the underlying jaw — and we do not offer adult skeletal expansion. Dr. Baharvand and Dr. Kang have managed narrow palate cases across the full spectrum, from Phase 1 expansion in young children to adult arch development cases that produce excellent outcomes within realistic expectations.
Dr. Baharvand and Dr. Kang are a husband-and-wife orthodontic team based in Frisco, with three convenient locations serving families across Frisco, The Colony, Prosper, and Little Elm. Dr. Baharvand is ABO board-certified and a published clinician whose work has appeared in the American Journal of Orthodontics and Dentofacial Orthopedics.
1,000+
Five-star reviews across 3 locations
ABO
Board-certified orthodontist
Published
AJO-DO cover clinician
Free
Consultation with full diagnostic records
Our Locations
5605 FM 423, Suite 600
Frisco, TX 75036
FM 423 & Lebanon Rd — next to the UPS Store
4713 Highway 121, Suite 304
The Colony, TX 75056
FM 423 & Hwy 121 — next to Ross
2155 University Dr, Suite 110
Frisco, TX 75033
On 380 across from Cook Children’s Medical Center Prosper
Hours: Mon–Fri 8:00am–5:00pm | 972.538.4343
Narrow Palate? Let’s Plan Treatment Right For Your Age.
Free consultations at all three Elate Orthodontics locations include a complete diagnostic workup: digital scans, panoramic X-rays, clinical photos, and an honest assessment of what palatal expansion or arch development can achieve at your specific age. We design treatment that produces real, lasting results within realistic expectations. No pressure, no surprises, no commitment to treatment.
Also see: All Conditions We Treat | Crossbite | Crowded Teeth | Palatal Expander | Airway Orthodontics | Before & After