Crowded Teeth Treatment in Frisco & The Colony, TX
Diagnosis & Correction by Dr. Baharvand & Dr. Kang — Expansion, Braces, Invisalign, Angel Aligners & Strategic Space Management
📞 972.538.4343
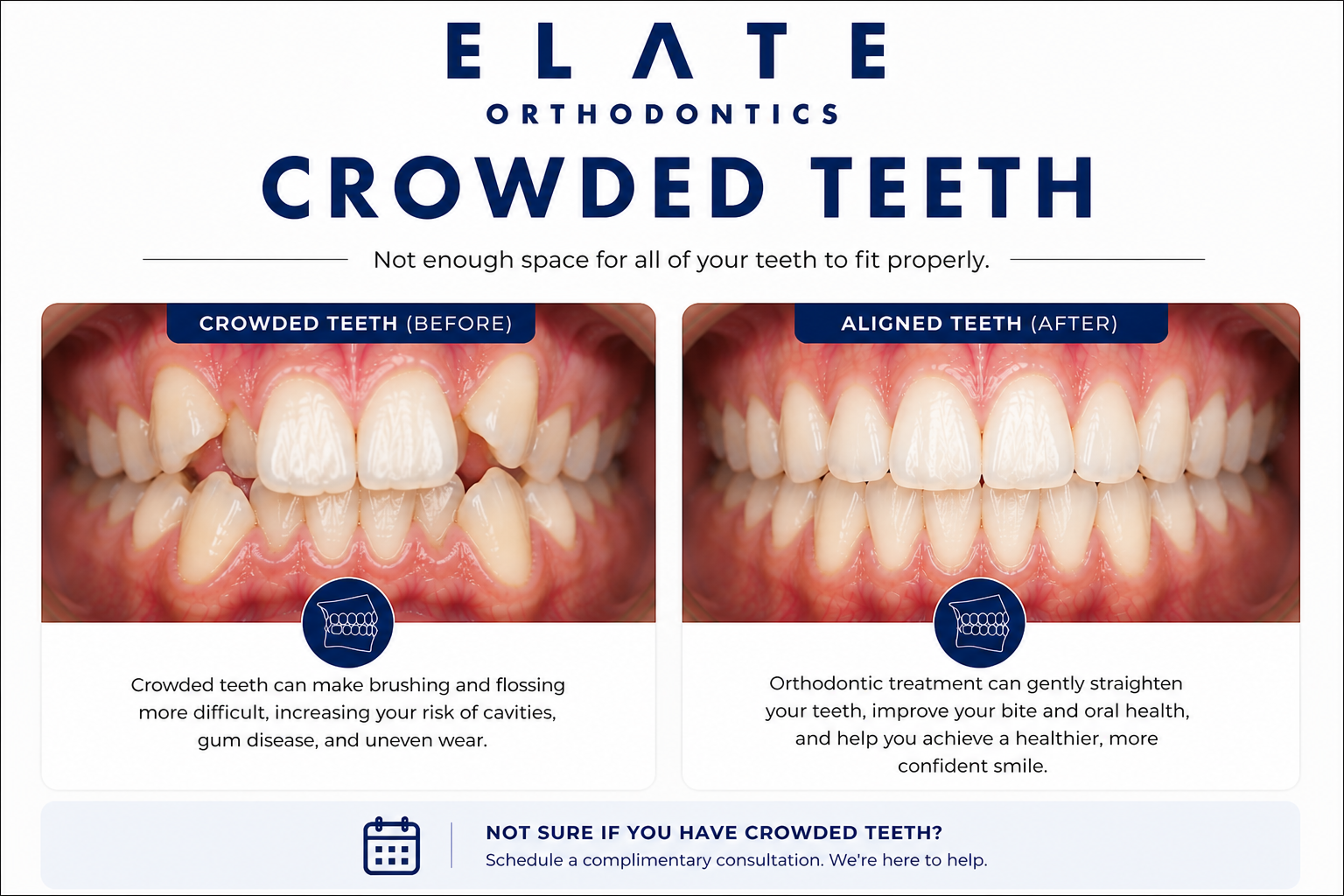
Crowded teeth correction at Elate Orthodontics — strategic space management for stable, long-term alignment
Crowded Teeth — Frisco & The Colony, TX
When the Teeth Outgrow the Jaw, Strategic Space Management Determines the Outcome
Crowded teeth is the most common malocclusion in orthodontics. It happens when there is not enough space in the dental arch for all the teeth to align side by side. Some teeth rotate. Some tip outward or inward. Some get blocked out of the arch entirely, particularly the upper canines and lower second premolars. The visible result is what most patients call “crooked teeth” — but the underlying issue is space. Solving crowded teeth means deciding how to create space for the teeth to align in healthy positions, and which teeth to keep, move, or in rare cases extract.
At Elate Orthodontics, Dr. Kevin Baharvand and Dr. Julia Kang treat crowded teeth in patients across Frisco, The Colony, Prosper, and Little Elm. The space management decision is one of the most important treatment plan decisions in orthodontics. The right approach depends on age, severity, jaw width, facial profile, and how much space is needed. We diagnose first, then design a plan that creates space in the way that best serves the long-term result. Done well, crowded teeth treatment produces stable, beautiful smiles that last for decades. Done poorly, the crowding returns within years.
As an ABO board-certified practice with a published clinician on staff, our diagnostic approach reflects the depth of training that distinguishes specialty orthodontic care. We take comprehensive records at every consultation and explain exactly what we see using your own digital scans, panoramic X-rays, and clinical photos. For crowded teeth cases, we measure the available space precisely and walk you through every option for creating the room your teeth need.
Mild, Moderate, or Severe — Severity Drives the Plan
Mild Crowding
Mild crowding involves up to about 3 millimeters of space deficiency — enough that a few teeth are slightly rotated or overlapping but the overall arch is close to ideal. Most adult late-stage crowding falls into this category, particularly the lower front teeth that have shifted over years. Mild cases are often treatable with clear aligners alone, sometimes with minor interproximal reduction (carefully smoothing tiny amounts of enamel between teeth) to create enough space. Treatment time is often short — 6 to 12 months in many adult cases.
Moderate Crowding
Moderate crowding involves 3 to 6 millimeters of space deficiency, with multiple teeth meaningfully out of position. This is the most common category we treat in teens and adults. Treatment usually combines comprehensive orthodontics (braces or aligners) with one or more space-creation strategies — palatal expansion in growing patients, interproximal reduction in adults, or repositioning of the bite. Comprehensive cases typically take 18 to 24 months.
Severe Crowding
Severe crowding involves more than 6 millimeters of space deficiency, often with teeth fully blocked out of the arch. Upper canines are particularly prone to becoming impacted in severe crowding cases. Treatment requires significant space creation, sometimes including selective extraction of premolars when expansion alone cannot provide enough room. We discuss extraction-vs-non-extraction tradeoffs honestly when severity warrants it.
Late Adult Lower Incisor Crowding
A specific pattern worth its own mention: many adults notice their lower front teeth becoming progressively more crowded in their 30s, 40s, and 50s. This is a combination of natural lower jaw forward growth, daily bite forces, and (for those who had braces years ago) inadequate retention. It is one of the most common reasons adults seek orthodontic retreatment and responds beautifully to focused short-course clear aligner therapy in 6 to 12 months. See our crooked teeth page for more on this adult pattern.
Severity classifications guide treatment planning but every case is individual. Comprehensive diagnosis identifies exactly how much space is needed and the best way to create it.
Underlying Causes
What Causes Crowded Teeth?
The most common cause of crowded teeth is genetic. Children often inherit a smaller jaw size from one parent and larger tooth size from the other, creating a mismatch where the teeth are simply too big for the arch. This is why crowding often runs in families and why we frequently see siblings with similar patterns.
Many crowded teeth cases stem from an upper jaw that has not developed wide enough during childhood. A narrow upper jaw produces a high arched palate, often coexists with crossbite, and forces the upper teeth to overlap or rotate. Catching a narrow jaw early — between ages 7 and 10 — allows palatal expansion to widen the arch and create space without extractions.
When children consistently breathe through the mouth, the tongue rests low rather than against the palate. Without normal tongue pressure shaping the upper jaw during growth, the jaw often develops narrower than it should — leading to crowding. We screen for airway and tongue posture issues during evaluation because addressing them is foundational for some growing patients.
When teeth are lost — whether baby teeth that fell out too early or adult teeth that were extracted in adolescence — neighboring teeth often drift into the empty space, creating crowding elsewhere in the arch. This is one of the most common causes of crowding in adults who have had teeth extracted earlier in life.
The lower jaw continues subtle forward growth into the 20s and beyond, and the daily forces of biting compound that pressure on the lower front teeth. This is why lower incisor crowding so often develops or worsens in adulthood. It is biological, not a sign that something went wrong with prior orthodontic treatment.
Many adults who had braces as teenagers see crowding return when retainers are not worn long-term. Teeth have a lifelong tendency to drift, and retention compliance is the single biggest factor in whether straight teeth stay straight. Relapse cases respond beautifully to focused short-course retreatment with clear aligners.
Why Crowded Teeth Are Worth Addressing
Many patients come to us focused on the cosmetic side of crowded teeth — that is a perfectly valid reason to pursue treatment. But crowding has real functional consequences that compound over years. Crowded teeth are harder to clean, accumulate more plaque between overlapping surfaces, and have higher rates of decay and gum disease as a direct result. Severely crowded teeth can also block out canines that then become impacted, requiring complex surgical and orthodontic coordination later.
For children, untreated crowding sometimes leads to extractions or surgical exposures in adolescence that could have been avoided with timely intervention during the growth window. For adults, late lower-incisor crowding tends to worsen progressively rather than improve. Either way, addressing crowding is one of the highest-return investments in long-term oral health.
What Untreated Crowding Causes
Higher rates of cavities and gum disease from overlapping surfaces that are difficult to clean
Impacted canines and other blocked-out teeth requiring surgical exposure later
Progressive worsening over time, particularly with adult lower-incisor crowding
Uneven tooth wear from teeth in non-ideal positions
Front teeth flaring outward from pressure of crowding behind them
Loss of the non-extraction window when severe crowding is left until adulthood
Self-consciousness about smile appearance affecting confidence in social and professional situations
Treatment Approach
How We Treat Crowded Teeth at Every Age
Crowded teeth treatment is fundamentally about creating space and then using that space well. The strategies for creating space differ dramatically by age, which is why early evaluation matters even when treatment is not yet needed.
Children (Ages 7–10) — The Expansion Window
This is the prime treatment window for crowding caused by a narrow upper jaw. A palatal expander can widen the upper jaw at the midpalatal suture before the bones fuse, creating physical space for the teeth to align without extractions. Phase 1 expansion in young children sometimes prevents the need for extractions in adolescence and dramatically simplifies later orthodontic treatment.
Not every crowded child needs Phase 1. We evaluate at age 7 and recommend treatment only when intervention will genuinely benefit the long-term outcome.
Teens (Ages 11–17)
The teen years are the most common treatment window for comprehensive crowding correction. Treatment uses braces or clear aligners combined with strategic space management — sometimes including expansion in younger teens, interproximal reduction, or selective extractions for severe cases. Most comprehensive teen cases take 18 to 24 months.
For teens with severely crowded canines that have become impacted, treatment is coordinated with an oral surgeon for surgical exposure and orthodontic traction.
Adults
Adult crowding treatment is one of the fastest-growing categories in our practice. Mild adult crowding — particularly late-stage lower incisor crowding — can often be corrected in 6 to 12 months with focused short-course clear aligner therapy combined with interproximal reduction. Moderate to severe cases use comprehensive treatment with braces or aligners.
In adults, the midpalatal suture is fused, so true skeletal expansion is no longer possible without surgical assistance. We work within the available arch and use space-creation strategies suited to the adult arch.
Space Management
How We Create Space for Crowded Teeth
The defining decision in crowded teeth treatment is how to create the space the teeth need. Each strategy has tradeoffs. The right combination depends on age, severity, and the long-term result we are working toward.
Widens the upper jaw to create physical space. The gold standard for crowding caused by a narrow upper jaw in growing children. Highly effective in patients ages 7 to 12, more limited in older teens and adults whose midpalatal suture has fused.
Carefully smoothing tiny amounts of enamel between teeth — typically 0.2 to 0.5 millimeters per contact — to create the space crowded teeth need. Done correctly, IPR is safe and well within the enamel thickness. It is the workhorse strategy for adult crowded teeth treatment.
Tipping teeth slightly outward to broaden the arch within the available bone. This works in mild cases where the arch shape can be improved without truly expanding the underlying jaw. Used commonly in adult treatment where palatal expansion is not an option.
For severe crowding cases where expansion and IPR cannot create enough space, removing a premolar from each quadrant provides significant room to align the remaining teeth properly. Reserved for cases where the long-term result is genuinely better with extractions than without. We discuss this honestly when severity warrants it.
In some teen and adult cases, removing impacted or partially erupted wisdom teeth (third molars) provides space and prevents pressure that drives lower incisor crowding. We coordinate with oral surgeons for these extractions when timing matters for the orthodontic plan.
Many comprehensive cases combine multiple approaches — palatal expansion plus mild IPR, or arch development combined with selective extractions. The strategy is sequenced based on growth status and what each phase will accomplish for the final result.
Treatment Options
Appliances We Use to Correct Crowding
Palatal Expander
The gold standard for crowding caused by a narrow upper jaw in growing children. Widens the upper jaw at the midpalatal suture, creating physical space for proper alignment. Often used as Phase 1 treatment, sometimes preventing extractions in adolescence.
Traditional Braces
The most versatile option for moderate to severe crowding. Braces give us precise control over each tooth and work well for cases combining crowding with bite correction, impacted teeth, or extraction therapy. The gold standard for the most demanding cases.
Clear Braces
Same effective mechanics as traditional braces with tooth-colored brackets that blend with natural enamel. A great option for teens and adults treating crowded teeth who want the predictability of braces with less visibility during treatment.
Invisalign
Modern Invisalign protocols handle the vast majority of mild to moderate crowding cases with excellent outcomes. Particularly effective for adult mild crowding and late lower-incisor crowding when combined with planned interproximal reduction. Aligners are removable for eating and brushing.
Angel Aligners
A clear aligner system we offer at Elate Orthodontics for appropriate cases. Like other clear aligner brands, Angel Aligners can correct mild to moderate crowding with treatment plans tailored to each patient’s anatomy and space requirements.
Pediatric Orthodontics (Phase 1)
Early interceptive treatment for growing children with developing crowding. Includes early space management, palatal expansion, and intercepting eruption issues. Catching crowding during the growth window can prevent extractions and simplify later treatment.
Permanent Bonded Retainers
For most crowding corrections, we recommend a small wire bonded behind the front teeth as a permanent retainer. This is invisible from the front, easy to maintain, and dramatically reduces the risk of late lower-incisor crowding returning over the years. Retention strategy is critical for keeping crowded teeth straight long-term.
Impacted Tooth Coordination
For severely crowded cases where canines or other teeth have become impacted, we coordinate with oral surgeons for surgical exposure and use orthodontic traction to bring the impacted tooth into the arch. Impaction management is a clinical specialty at our practice.
AAO Recommendation
Crowding Caught Early Sometimes Prevents Extractions Later
The American Association of Orthodontists recommends an evaluation by age 7. For crowded teeth, the early evaluation lets us identify cases where palatal expansion during the active growth window can create enough space to avoid extractions in adolescence. This is one of the strongest practical reasons for the age-7 evaluation. Severe crowding caught at age 8 to 10 often responds beautifully to expansion. The same case caught at age 16 may require premolar extractions to correct fully.
For adults, the right time for crowded teeth treatment is when you decide you want it addressed. Modern adult orthodontics — particularly clear aligners with planned interproximal reduction — produces excellent outcomes at any age, with minimal visibility during the months of treatment.
See Real Outcomes
Crowded Teeth Cases From Our Practice
Our before-and-after gallery includes real crowded teeth corrections at Elate Orthodontics, ranging from Phase 1 expansion cases that avoided later extractions, to teen comprehensive cases corrected with braces, to adult lower-incisor crowding corrected with short-course clear aligners. Each case shows the diagnosis, the appliances used, and the final result.
Common Questions
Crowded Teeth FAQ
In most cases, no. The vast majority of crowded teeth cases can be treated without extractions using palatal expansion in growing children, interproximal reduction in adults, or arch development. Selective premolar extractions are reserved for severe crowding where expansion and other strategies cannot create enough space. We discuss extraction-vs-non-extraction tradeoffs honestly when severity warrants it.
Yes — modern Invisalign protocols handle the vast majority of mild to moderate crowding cases. For severe crowding requiring extractions or significant skeletal correction, traditional braces often produce more predictable results. Adult mild crowding (especially late lower-incisor crowding) is one of the best applications for short-course clear aligner therapy, often completed in 6 to 12 months.
Late lower-incisor crowding is real and very common. The lower jaw continues subtle forward growth into the 20s and beyond, and daily bite forces gradually crowd the lower front teeth. If you had braces years ago and stopped wearing your retainer, this drift includes orthodontic relapse. Either way, focused short-course treatment with clear aligners typically addresses it in 6 to 12 months with permanent retention to prevent recurrence.
Interproximal reduction is the careful smoothing of tiny amounts of enamel between teeth — typically 0.2 to 0.5 millimeters per contact — to create space for crowded teeth to align. Done correctly, IPR is well within the thickness of the enamel and is completely safe. It is the workhorse strategy for adult crowded teeth treatment and is performed routinely throughout orthodontic care.
Mild adult crowding can sometimes be completed in 6 to 12 months. Moderate crowding typically takes 12 to 18 months. Severe cases involving extractions or impacted teeth usually take 18 to 30 months. Phase 1 expansion in young children typically takes 9 to 14 months, with a second phase of comprehensive treatment in adolescence if needed.
Most PPO dental insurance plans include orthodontic benefits that apply to crowded teeth treatment. Coverage varies by plan, with some covering teen treatment more generously than adult treatment. We are in-network with most major PPO carriers and offer flexible financing through Cherry to make treatment accessible regardless of insurance coverage.
Why Frisco & The Colony Patients Choose Elate Orthodontics for Crowded Teeth
Crowded teeth treatment is fundamentally about good space management decisions. The depth of the diagnosis, the experience to know when expansion can avoid extractions, and the willingness to discuss extraction-vs-non-extraction tradeoffs honestly are what separate good outcomes from great ones. Dr. Baharvand and Dr. Kang have managed thousands of crowded teeth cases across the full spectrum, from Phase 1 expansion in elementary school children to complex adult cases combining expansion alternatives, IPR, and selective extractions.
Dr. Baharvand and Dr. Kang are a husband-and-wife orthodontic team based in Frisco, with three convenient locations serving families across Frisco, The Colony, Prosper, and Little Elm. Dr. Baharvand is ABO board-certified and a published clinician whose work has appeared in the American Journal of Orthodontics and Dentofacial Orthopedics.
1,000+
Five-star reviews across 3 locations
ABO
Board-certified orthodontist
Published
AJO-DO cover clinician
Free
Consultation with full diagnostic records
Our Locations
5605 FM 423, Suite 600
Frisco, TX 75036
FM 423 & Lebanon Rd — next to the UPS Store
4713 Highway 121, Suite 304
The Colony, TX 75056
FM 423 & Hwy 121 — next to Ross
2155 University Dr, Suite 110
Frisco, TX 75033
On 380 across from Cook Children’s Medical Center Prosper
Hours: Mon–Fri 8:00am–5:00pm | 972.538.4343
Crowded Teeth? Let’s Find the Right Way to Make Room.
Free consultations at all three Elate Orthodontics locations include a complete diagnostic workup: digital scans, panoramic X-rays, clinical photos, and precise measurement of how much space your teeth need. We walk you through every option for creating that space and design a treatment plan that produces stable, lasting results. No pressure, no surprises, no commitment to treatment.
Also see: All Conditions We Treat | Crooked Teeth | Gapped Teeth | Impacted Teeth | Before & After