Tongue Thrust Treatment in Frisco & The Colony, TX
Diagnosis & Correction by Dr. Baharvand & Dr. Kang — Habit Appliances, Myofunctional Therapy, Plus Braces, Invisalign & Angel Aligners
📞 972.538.4343
Tongue thrust treatment at Elate Orthodontics — addressing the habit and the structural changes it causes
Tongue Thrust — Frisco & The Colony, TX
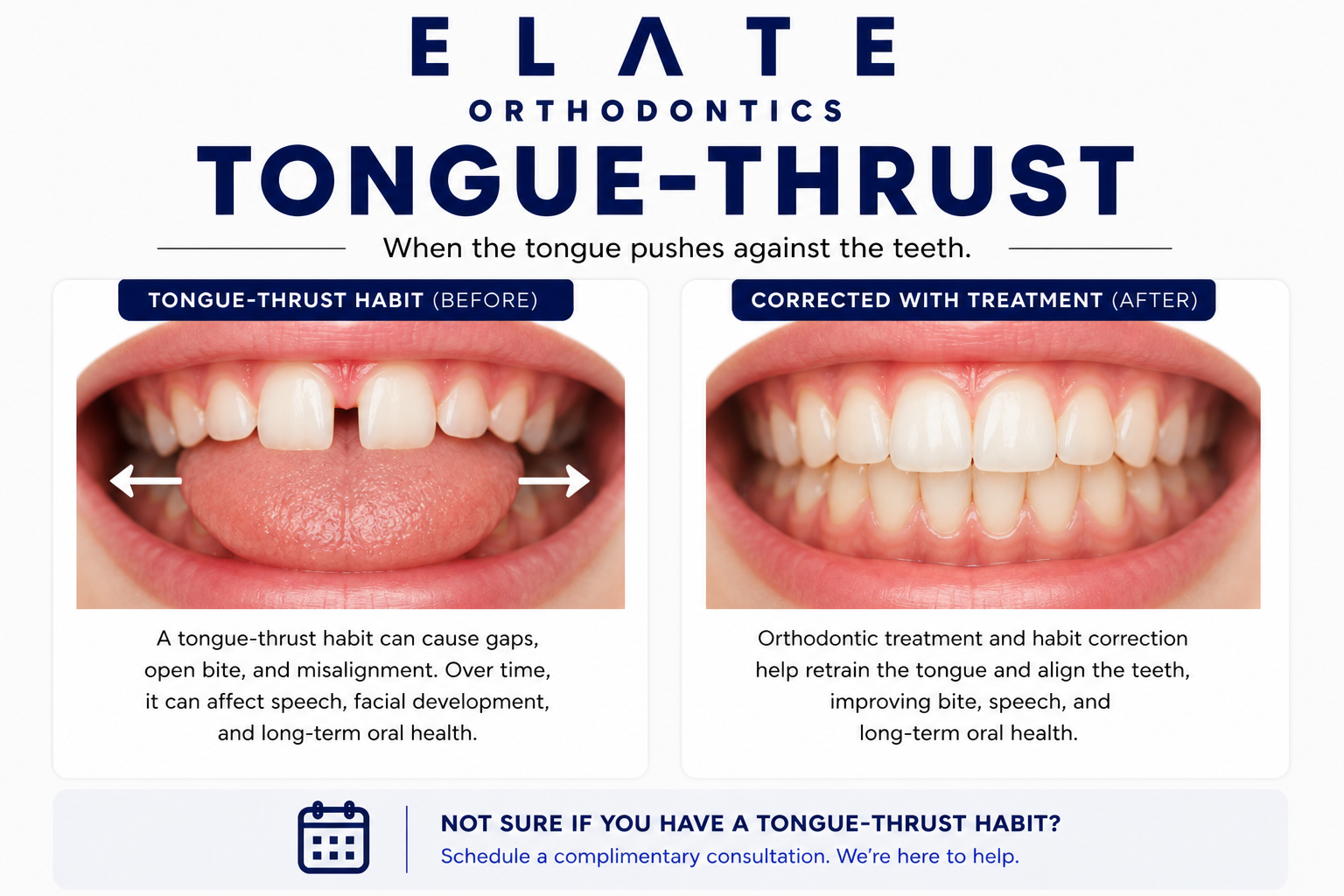
Tongue Thrust Is Often the Hidden Driver Behind Open Bite, Gapped Teeth, and Orthodontic Relapse
Tongue thrust refers to the habit of pushing the tongue forward against or between the front teeth during swallowing or at rest. The tongue is one of the most powerful forces shaping the dental arches throughout life. The average person swallows around a thousand times per day, and each swallow with an abnormal tongue posture exerts pressure that can shift teeth forward, create open bites, widen gaps, and undo years of orthodontic treatment if the habit is not addressed alongside the alignment.
At Elate Orthodontics, Dr. Kevin Baharvand and Dr. Julia Kang treat tongue thrust in patients across Frisco, The Colony, Prosper, and Little Elm. Tongue thrust is rarely the primary reason patients come to us. It is usually the hidden driver behind something else they have noticed: an open bite that will not close, gaps that keep coming back, flaring upper front teeth, or relapse after prior orthodontic treatment. We screen for tongue thrust in every new patient evaluation because addressing it is often the difference between treatment that lasts and treatment that fails.
As an ABO board-certified practice with a published clinician on staff, our diagnostic approach reflects the depth of training that distinguishes specialty orthodontic care. We take comprehensive records at every consultation and explain exactly what we see using your own digital scans, panoramic X-rays, and clinical photos. For tongue thrust cases, we combine orthodontic correction with habit appliances and coordination with myofunctional therapists when needed, because retraining the tongue is essential for stable long-term results.
The Common Patterns of Tongue Thrust
Anterior Tongue Thrust
The most common pattern. The tongue pushes forward against the upper or lower front teeth, or between them, during swallowing and often at rest. Anterior tongue thrust is the underlying habit driver for most tongue-thrust-related open bites and front tooth flaring. Many patients are unaware they have this habit until it is pointed out during examination.
When patients with anterior tongue thrust are asked to swallow with their mouth open, the tongue is visibly seen pushing forward between the front teeth. This is one of the diagnostic checks we perform during evaluation.
Lateral Tongue Thrust
Less common but clinically important. The tongue pushes sideways against the back teeth on one or both sides during swallowing or at rest. Lateral tongue thrust can produce a posterior open bite where the back teeth on one side do not meet, or it can prevent posterior open bites from closing after orthodontic treatment.
Lateral tongue thrust often coexists with airway issues or anatomic variation. Treatment requires habit modification combined with appropriate orthodontic correction.
Low Tongue Posture
The tongue rests on the floor of the mouth rather than against the palate. While not technically a thrust, low tongue posture has many of the same downstream effects. The tongue is one of the strongest forces shaping the upper jaw during growth — without normal contact between the tongue and the palate, the upper jaw often develops narrow, contributing to crowding and crossbite.
Low tongue posture is most common in patients with chronic mouth breathing, large tonsils or adenoids, or tongue-tie. We screen for these factors during evaluation.
Tongue Thrust with Mouth Breathing
Many patients with tongue thrust also chronically mouth-breathe. The two conditions reinforce each other — chronic mouth breathing requires the tongue to drop low to allow airflow, which then sets up the muscle pattern that produces tongue thrust during swallowing. Treating one without addressing the other often produces incomplete results.
For patients with combined tongue thrust and mouth breathing, we coordinate with ENT specialists, allergists, and myofunctional therapists alongside orthodontic treatment. Our airway orthodontics page covers this connection in more depth.
Most patients have a combination of these patterns. Diagnosing the specific tongue posture and movement is essential for designing treatment that prevents relapse.
Underlying Causes
What Causes Tongue Thrust?
All infants swallow with a tongue-forward pattern, which is normal during nursing. The mature swallow pattern (tongue against the palate, teeth gently together) typically develops between ages 4 and 6 as children transition from soft to solid foods. When this transition does not occur fully, the infant pattern persists into childhood and becomes the chronic tongue thrust pattern we see in older children and adults.
Children who continue thumb sucking or pacifier use past age 4 to 5 often develop persistent tongue thrust patterns. The thumb or pacifier holds the tongue in a forward position during early development, and the muscle memory persists even after the habit stops. Stopping the habit alone is often not enough — the resulting tongue thrust may need separate treatment.
Mouth breathing forces the tongue to drop down to allow airflow through the oral cavity, which sets up an abnormal resting position. Over time, this becomes the default tongue posture during swallowing as well. Mouth breathing in children is one of the strongest predictors of persistent tongue thrust into adulthood.
Chronically enlarged tonsils and adenoids force children to mouth breathe and adopt a low tongue posture. This in turn produces tongue thrust during swallowing. Identifying and addressing tonsil and adenoid issues with an ENT specialist alongside orthodontic treatment produces better outcomes than addressing the orthodontic component alone.
A restrictive frenum under the tongue can prevent it from reaching the palate during swallowing, producing a forward thrust pattern as a compensatory motion. We screen for tongue-tie during evaluation, and when significant, coordinate with appropriate specialists for frenectomy. Tongue-tie release may be an essential first step before myofunctional retraining can succeed.
Children with chronic environmental allergies or recurrent sinus issues often default to mouth breathing because nasal breathing is uncomfortable. Years of mouth breathing during growth set up the tongue posture and swallowing patterns that produce chronic tongue thrust. Coordinating with allergists is part of comprehensive care for these patients.
Why Tongue Thrust Matters for Treatment Stability
Tongue thrust is one of the most common reasons orthodontic treatment relapses. A patient with untreated tongue thrust who completes braces or aligners may have a beautiful smile at the end of treatment, only to watch the front teeth gradually drift forward, gaps reopen, or the open bite return over the following years. The tongue applies pressure thousands of times per day, and that pressure does not stop just because the orthodontic treatment is done.
This is why we screen for tongue thrust in every new patient evaluation and address it as part of the treatment plan from the start. For patients with significant tongue thrust, treatment that does not include habit modification has a high relapse rate. The honest conversation about the tongue’s role in stability is part of what we do at consultation.
What Untreated Tongue Thrust Causes
Anterior open bite (front teeth not meeting when biting down) that often does not close on its own
Flaring of upper front teeth from constant forward pressure
Reopening of gaps after orthodontic gap closure (one of the most common causes of diastema relapse)
Speech difficulties, particularly with lisping (S, Z, T, D, N, L sounds)
Orthodontic relapse after braces or aligners as teeth drift back toward their pre-treatment positions
Contribution to narrow palate development in children with low tongue posture
Difficulty achieving stable retention even with permanent retainers when the underlying habit is not addressed
Treatment Approach
How We Treat Tongue Thrust at Every Age
Tongue thrust treatment is fundamentally about retraining a muscle pattern that has been reinforced thousands of times per day for years. Effective treatment combines awareness, behavioral retraining, sometimes habit appliances, and orthodontic correction of the structural changes the habit has caused. The right combination depends on age and severity.
Children (Ages 7–10)
Younger children respond well to habit retraining when the tongue thrust is identified early, before structural changes become severe. Treatment often combines habit appliances (small devices that gently remind the tongue to stay back) with myofunctional therapy exercises. For children with contributing airway issues, ENT or allergy coordination is essential.
Catching tongue thrust at this age can sometimes prevent the development of open bite and other downstream issues entirely.
Teens (Ages 11–17)
Teens with tongue thrust typically have established structural changes (open bite, flared front teeth, gaps) that require comprehensive orthodontic treatment alongside habit modification. We integrate habit appliances or myofunctional therapy into the orthodontic plan from the start, because correcting the structure without correcting the habit usually leads to relapse.
Comprehensive treatment with combined approaches typically takes 18 to 24 months, with myofunctional therapy continuing for several months after braces or aligners are removed.
Adults
Adult tongue thrust is more challenging than pediatric cases because the muscle pattern has been reinforced for decades, but treatment is highly effective when patients are committed to the retraining process. Adults often come to us with relapse from prior orthodontic treatment, persistent open bites, or recurring gaps that no one previously identified as tongue-thrust-driven.
Treatment combines myofunctional therapy with comprehensive orthodontic correction. Patient commitment to the daily exercises is the variable that determines whether long-term stability is achieved.
Treatment Options
Treatments We Use to Address Tongue Thrust
Myofunctional Therapy Coordination
The cornerstone of tongue thrust treatment. Myofunctional therapists are trained specialists who teach exercises to retrain tongue posture and swallowing patterns. Treatment typically involves daily exercises practiced over several months. We coordinate with myofunctional therapists in the Frisco area and integrate their care plans into our orthodontic timeline.
Habit Appliances (Tongue Cribs & Reminders)
Small fixed appliances that block the tongue from pushing forward against the front teeth, providing a constant physical reminder to keep the tongue in the proper position. Habit appliances work alongside myofunctional therapy to interrupt the pattern and allow new muscle memory to form. Used selectively for cases where additional support is needed.
Traditional Braces
For correcting the structural changes tongue thrust has caused — open bite, flared front teeth, gaps. Braces give us precise control over each tooth and remain the most reliable option when comprehensive treatment is needed alongside habit modification.
Clear Braces
Same effective mechanics as traditional braces with tooth-colored brackets. A great option for teens and adults treating tongue-thrust-related structural issues who want the predictability of braces with less visibility during treatment.
Invisalign
Modern Invisalign protocols handle most tongue-thrust-related structural issues effectively. The aligners themselves provide a partial physical reminder to keep the tongue back during swallowing because they cover the teeth. Combined with myofunctional therapy, Invisalign is often a strong option for adult tongue thrust cases.
Angel Aligners
A clear aligner system we offer at Elate Orthodontics for appropriate cases. Like other clear aligner brands, Angel Aligners can correct tongue-thrust-related structural changes in adult cases when combined with myofunctional therapy and consistent retention.
Permanent Bonded Retainers
For tongue thrust patients, permanent bonded retainers behind the front teeth provide essential resistance to the daily forward pressure of the tongue. These small wires are invisible from the front, easy to maintain, and dramatically reduce the chance of relapse compared to removable retainers alone. Standard recommendation for tongue thrust cases.
ENT, Allergy & Tongue-Tie Coordination
When tongue thrust is driven by enlarged tonsils and adenoids, chronic allergies, or restrictive tongue-tie, addressing those underlying factors is part of comprehensive care. We coordinate with ENT specialists, allergists, and clinicians who manage tongue-tie release. Treating the orthodontic component without addressing the underlying driver often produces incomplete results.
AAO Recommendation
Catching Tongue Thrust Early Often Prevents the Open Bite It Would Cause
The American Association of Orthodontists recommends an evaluation by age 7. For tongue thrust, this matters because the habit pattern is most easily retrained before significant structural changes have developed. A child whose tongue thrust is identified at age 7 and addressed with early myofunctional therapy and habit modification often does not develop the open bite or flared front teeth that the same untreated habit would have caused by age 12.
For adults, tongue thrust is one of the most commonly missed diagnoses in patients with orthodontic relapse. If you have noticed your front teeth gradually moving forward, gaps reopening, or your old open bite returning despite wearing your retainer, tongue thrust may be the underlying cause. We diagnose this honestly during evaluation and design treatment that addresses both the structure and the habit.
See Real Outcomes
Tongue Thrust Cases From Our Practice
Our before-and-after gallery includes real tongue thrust cases at Elate Orthodontics, ranging from early Phase 1 cases that prevented open bite development, to teen comprehensive cases combining orthodontic correction with myofunctional therapy, to adult retreatment cases addressing relapse from prior treatment that had not identified the underlying tongue habit. Each case shows the diagnosis, the appliances used, and the final result.
Common Questions
Tongue Thrust FAQ
Common signs include an anterior open bite (front teeth not meeting when biting down), front teeth that are flaring forward, gaps that have reopened after orthodontic treatment, lisping with S or Z sounds, and noticing your tongue pushing against your front teeth when you swallow. A clear diagnostic test is to swallow with your lips parted and observe whether the tongue pushes forward against or between the front teeth.
No. Braces or aligners can correct the structural changes tongue thrust has caused, but they do not address the underlying muscle pattern. If the tongue continues pushing forward thousands of times per day after braces are removed, the teeth will gradually drift back toward their pre-treatment positions. This is why we combine orthodontic treatment with myofunctional therapy or habit appliances when tongue thrust is present.
Myofunctional therapy is a structured program of exercises taught by a trained specialist to retrain the muscles of the tongue, lips, and face. The goal is to establish proper tongue posture (resting against the palate) and swallow patterns (tongue against the palate, teeth gently together). Treatment typically involves daily exercises practiced over several months. We coordinate with myofunctional therapists in the Frisco area as part of comprehensive tongue thrust care.
Yes, though it requires consistent commitment to daily exercises over several months. Adults can absolutely change tongue posture and swallow patterns, but the muscle pattern has been reinforced for decades, so the retraining process takes longer than in children. Patients who commit to myofunctional therapy alongside their orthodontic treatment achieve excellent stability long-term.
This is one of the classic patterns of untreated tongue thrust. If your open bite returned after orthodontic treatment, there is a strong chance that tongue thrust was the underlying cause and was not addressed during the original treatment. Retreatment combined with myofunctional therapy and permanent bonded retainers typically produces stable results when the tongue habit is finally addressed. We diagnose this specifically during retreatment consultations.
Orthodontic treatment portions are typically covered by PPO dental insurance plans that include orthodontic benefits. Myofunctional therapy is sometimes covered separately under medical insurance for documented functional issues, though coverage varies significantly by plan. We help patients understand what each component is likely to cost and offer flexible financing through Cherry to make comprehensive care accessible.
Why Frisco & The Colony Patients Choose Elate Orthodontics for Tongue Thrust
Tongue thrust is the most commonly missed diagnosis in adult orthodontic relapse. The willingness to look for it during evaluation, the experience to recognize the patterns it produces, and the discipline to coordinate with myofunctional therapists are what separate good outcomes from great ones. Dr. Baharvand and Dr. Kang screen for tongue thrust in every comprehensive evaluation and integrate habit modification into treatment plans from the start when it is identified.
Dr. Baharvand and Dr. Kang are a husband-and-wife orthodontic team based in Frisco, with three convenient locations serving families across Frisco, The Colony, Prosper, and Little Elm. Dr. Baharvand is ABO board-certified and a published clinician whose work has appeared in the American Journal of Orthodontics and Dentofacial Orthopedics.
1,000+
Five-star reviews across 3 locations
ABO
Board-certified orthodontist
Published
AJO-DO cover clinician
Free
Consultation with full diagnostic records
Our Locations
5605 FM 423, Suite 600
Frisco, TX 75036
FM 423 & Lebanon Rd — next to the UPS Store
4713 Highway 121, Suite 304
The Colony, TX 75056
FM 423 & Hwy 121 — next to Ross
2155 University Dr, Suite 110
Frisco, TX 75033
On 380 across from Cook Children’s Medical Center Prosper
Hours: Mon–Fri 8:00am–5:00pm | 972.538.4343
Tongue Thrust? Let’s Address the Habit and the Bite Together.
Free consultations at all three Elate Orthodontics locations include a complete diagnostic workup: digital scans, panoramic X-rays, clinical photos, and screening for tongue thrust patterns that may be driving your concerns. We design treatment that addresses both the structural changes and the underlying muscle habit. No pressure, no surprises, no commitment to treatment.
Also see: All Conditions We Treat | Open Bite | Gapped Teeth | Protruding Teeth | Narrow Palate | Airway Orthodontics | Before & After