Underbite Treatment in Frisco & The Colony, TX
Diagnosis, Causes & Correction by Dr. Baharvand & Dr. Kang — Early Intervention, Braces, Invisalign & Surgical Coordination
📞 972.538.4343
Underbite correction at Elate Orthodontics — diagnosed early when treatment options are widest
Underbite — Frisco & The Colony, TX
When the Lower Teeth Sit in Front of the Upper Teeth, Timing Matters More Than Anything
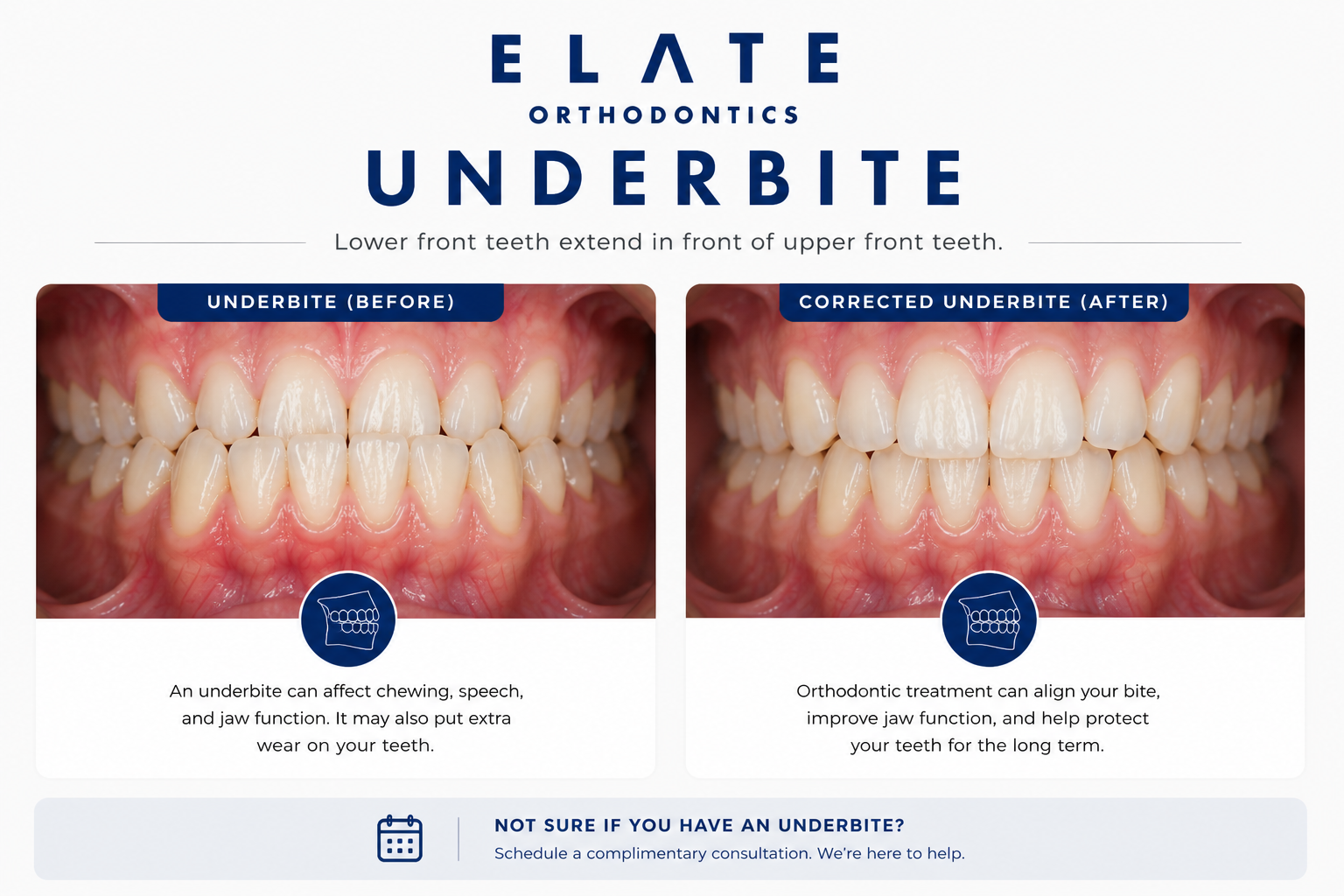
An underbite is a bite condition where the lower front teeth sit in front of the upper front teeth when biting down. It is the opposite of an overbite. Sometimes called a Class III malocclusion or prognathism, an underbite can range from a single tooth in crossbite to a fully reversed bite where the entire lower jaw projects past the upper jaw. Underbites are most often skeletal in nature, meaning the issue is not just the teeth but the size and position of the jaws themselves.
At Elate Orthodontics, Dr. Kevin Baharvand and Dr. Julia Kang treat underbites in patients across Frisco, The Colony, Prosper, and Little Elm. Of all the bite conditions we manage, underbite is the one where early evaluation matters the most. A skeletal underbite caught at age 7 to 9 can often be corrected without surgery using a reverse-pull headgear or similar appliance. The same case caught at age 25 may require jaw surgery to correct fully. The biology of growth gives us a window, and that window closes earlier than most parents realize.
As an ABO board-certified practice with a published clinician on staff, our diagnostic approach reflects the depth of training that distinguishes specialty orthodontic care. We take comprehensive records at every consultation and explain exactly what we see using your own digital scans, panoramic X-rays, and clinical photos. For underbite cases, identifying the cause early changes the entire treatment plan.
Skeletal vs. Dental Underbite (And Why the Difference Matters)
Skeletal Underbite
A skeletal underbite means the upper jaw, the lower jaw, or both are positioned incorrectly relative to each other at the bone level. The most common pattern is a small or recessed upper jaw that has not grown forward enough. Less commonly, the lower jaw has grown too far forward. Skeletal underbites are usually genetic and run in families.
The treatment for a skeletal underbite depends entirely on age. In growing children, we can guide the upper jaw forward using a reverse-pull headgear, often paired with a palatal expander. In adults, the same skeletal pattern typically requires either orthodontic camouflage or coordination with an oral surgeon for jaw surgery.
Dental Underbite (Anterior Crossbite)
A dental underbite, sometimes called an anterior crossbite, occurs when the jaws are reasonably aligned but one or more of the upper front teeth are tipped backward or sit behind the lower teeth. The skeletal foundation is normal. The teeth themselves are simply in the wrong position.
Dental underbites are usually simpler to correct with braces or clear aligners and do not require growth modification or surgery. They still benefit from early treatment, since an upper tooth biting behind a lower tooth can cause uneven jaw growth and force the lower jaw into a forward shift over time, eventually creating a skeletal pattern that did not exist before.
Diagnosing whether an underbite is skeletal, dental, or a combination determines the entire treatment plan. This is why a specialist’s diagnosis matters.
Underlying Causes
What Causes an Underbite?
Underbite has the strongest genetic component of any bite condition. If one or both parents had an underbite, their children have a meaningfully higher likelihood of developing one. Even without a family history, jaw shape is largely inherited, and small variations in jaw growth can express as an underbite.
The most common skeletal pattern in underbite cases is an upper jaw that has not grown forward enough during development. The lower jaw is normally positioned, but the upper jaw is set back, creating the appearance of a protruding lower jaw. This pattern responds beautifully to reverse-pull headgear when caught early.
Less commonly, the lower jaw grows more than expected, projecting forward past the upper jaw. This pattern is harder to address with growth modification because we cannot easily slow lower jaw growth. Severe cases of mandibular prognathism are typically treated with jaw surgery in adulthood.
Sometimes one or more upper front teeth simply erupt tipped behind the lower teeth, creating an anterior crossbite. The jaws are well-positioned, but the tooth angulation is wrong. Often caused by lingering baby teeth, tooth size discrepancies, or eruption path issues.
In some children, the bite appears as an underbite because the lower jaw shifts forward to avoid an interference with an upper tooth. The skeletal relationship may actually be normal, but the patient functions in an underbite position. These cases need careful diagnosis because correcting the interference often resolves the bite without major intervention.
Patients born with cleft lip and palate often develop an underbite due to scarring from early surgical repairs that restricts upper jaw growth. These cases require coordinated care between orthodontists, oral surgeons, and the cleft team. We work closely with cleft teams when these patients are referred to us.
Why an Untreated Underbite Is Worth Addressing Early
Underbite is unique among the bite conditions because the treatment window narrows dramatically with age. A child with a skeletal underbite at age 8 has options that simply do not exist for the same patient at age 18. The reverse-pull headgear works because the bones of the upper jaw have not yet fused. Once they fuse, that option is off the table.
Beyond the timing issue, untreated underbites cause real functional and cosmetic problems that compound over years. The earlier we catch them, the better the outcome and the less invasive the treatment.
What Happens If Underbite Is Left Untreated
Progressive worsening of the bite as the lower jaw continues to grow during adolescence
Difficulty biting and chewing certain foods, particularly anything that requires the front teeth
Speech difficulties, particularly with sounds that require front-tooth contact
Accelerated and uneven wear on the front teeth
Asymmetric facial growth when the underbite is one-sided
TMJ strain from chronic compensation in jaw position
Loss of the non-surgical treatment window, meaning what could be corrected with a headgear in childhood may require jaw surgery in adulthood
Self-consciousness about facial profile and smile appearance
Treatment Approach
How We Treat Underbite at Every Age
No bite condition shows a more dramatic difference between early and late treatment than underbite. The treatment options at age 8 are different from age 14, and very different from age 25. This is why we strongly support the AAO recommendation for evaluation by age 7.
Children (Ages 7–10) — The Best Window
This is the prime treatment window for skeletal underbites. The bones of the upper jaw have not yet fused at the midpalatal suture, and the upper jaw can be expanded and pulled forward using a reverse-pull headgear (also called a face mask). This appliance is worn at night and slowly brings the upper jaw forward to meet the lower jaw, often eliminating the need for surgery later.
Phase 1 treatment for underbite typically lasts 9 to 14 months, with a second phase of braces or aligners in adolescence to fine-tune tooth position once permanent teeth are in.
Teens (Ages 11–17)
For mild to moderate underbites in teens, braces or clear aligners with strategic elastics can correct the bite by tipping teeth into a healthier relationship. The midpalatal suture has often fused or is fusing, making reverse-pull less effective for purely skeletal correction, though some growth-active patients still benefit from a combined approach.
For severe skeletal underbites in teens, we sometimes recommend monitoring growth and planning for combined orthodontic and surgical treatment in late adolescence once growth is complete.
Adults
In adults, underbite treatment falls into two paths. Mild to moderate dental underbites and some milder skeletal cases can be camouflaged with braces or clear aligners that tip the teeth into a corrected position, sometimes with selective extractions. This is called orthodontic camouflage.
For severe skeletal underbites where camouflage will not produce a stable, healthy bite, the only complete solution is orthognathic (jaw) surgery combined with orthodontic treatment. We coordinate with experienced oral surgeons for these cases and walk you through every step honestly. We will tell you clearly which path is realistic for your case.
Treatment Options
Treatments We Use to Correct Underbite
Reverse-Pull Headgear (Face Mask)
The gold standard for early skeletal underbite treatment. Worn primarily at night, the face mask gently pulls the upper jaw forward during the active growth window. Combined with a palatal expander, this appliance can correct skeletal underbites in growing children and often eliminates the need for surgery later.
Palatal Expander
Frequently used alongside a reverse-pull headgear in young patients. Widening the upper jaw creates space for proper alignment and disengages the bite, allowing the upper jaw to move forward more easily. A workhorse appliance in early underbite treatment.
Traditional Braces
The most versatile option for underbite correction in teens and adults. Braces give us precise control over tooth movement and work well with elastics that pull the upper teeth forward and the lower teeth back. The gold standard for complex orthodontic camouflage and for finishing surgical cases.
Clear Braces
Same effective mechanics as traditional braces with tooth-colored brackets. A great option for teens and adults treating mild to moderate underbites who want the predictability of braces with less visibility during treatment.
Invisalign
Clear aligners can correct mild to moderate dental underbites in cooperative patients. With Class III elastics and precision attachments, modern Invisalign protocols are effective for the right candidates. Severe skeletal cases typically require braces or surgical coordination instead.
Angel Aligners
A clear aligner system we offer at Elate Orthodontics for appropriate cases. Like other clear aligner brands, Angel Aligners can correct mild to moderate dental underbites with a treatment plan tailored to each patient’s specific anatomy.
Orthognathic Surgery (Severe Adult Cases)
For adults with severe skeletal underbites where orthodontic treatment alone cannot produce a stable, healthy bite, we coordinate with experienced oral surgeons for jaw surgery combined with orthodontic treatment. This is reserved for cases that genuinely require it. Surgical underbite correction is one of the most transformative treatments in orthodontics, both functionally and aesthetically.
AAO Recommendation
Underbite Is the Most Time-Sensitive Bite Condition
The American Association of Orthodontists recommends an evaluation by age 7. For underbite, this recommendation is particularly important. The reverse-pull headgear works because it acts on bone that is still developing. Once the upper jaw bones fuse, typically between ages 11 and 13, this option becomes far less effective. The same skeletal underbite that responds well to a face mask at age 8 may require jaw surgery at age 25.
If you suspect your child has an underbite, or if a pediatric dentist has flagged an anterior crossbite, do not wait. An evaluation does not commit you to treatment. It simply identifies whether and when intervention will help.
See Real Outcomes
Underbite Cases From Our Practice
Our before-and-after gallery includes real underbite corrections at Elate Orthodontics, ranging from early Phase 1 cases corrected with reverse-pull and expansion to adult cases corrected with braces or surgical coordination. Each case shows the diagnosis, the appliances used, and the final result.
Common Questions
Underbite FAQ
Skeletal underbites should be evaluated and treated as early as ages 7 to 9 when indicated. This is the window when reverse-pull headgear can guide the upper jaw forward without surgery. Waiting until adolescence or adulthood often eliminates the non-surgical option for skeletal cases. Dental underbites can be treated at any age, but earlier is still better to prevent compensatory growth changes.
Yes, in most cases when caught early. Skeletal underbites in growing children respond well to reverse-pull headgear and palatal expansion, often eliminating the need for surgery. Mild to moderate underbites in teens and adults can usually be corrected with braces or aligners using orthodontic camouflage. Surgery is reserved for severe skeletal cases in adults where orthodontic treatment alone cannot create a stable, healthy bite.
Yes, for mild to moderate dental underbites in cooperative patients. Modern Invisalign protocols use Class III elastics and precision attachments to tip teeth into corrected positions. For severe skeletal underbites or cases requiring growth modification, traditional braces or surgical coordination usually produce more reliable results.
In most cases, yes. The lower jaw continues to grow throughout adolescence, often after upper jaw growth has slowed. A skeletal underbite that looks mild at age 8 frequently worsens during the pubertal growth spurt. This is why early evaluation matters and why Phase 1 treatment is so often recommended for these cases.
Phase 1 treatment for skeletal underbites in young children typically takes 9 to 14 months, followed by monitoring and a second phase of braces or aligners in adolescence. Adult orthodontic camouflage cases generally take 18 to 30 months. Combined surgical and orthodontic treatment can take 18 to 36 months total, depending on the complexity of the case.
Most PPO dental insurance plans include orthodontic benefits that apply to underbite treatment, especially when there is a documented functional concern. Coverage varies by plan. We are in-network with most major PPO carriers and offer flexible financing through Cherry to make treatment accessible regardless of insurance coverage. For surgical cases, medical insurance may cover the surgical portion when medically necessary.
Why Frisco & The Colony Families Choose Elate Orthodontics for Underbite Correction
Underbite is one of the most timing-sensitive conditions in orthodontics. The depth of the diagnosis, the experience to know when to intervene early, and the willingness to coordinate with oral surgeons for adult cases are what separate good outcomes from great ones. Dr. Baharvand and Dr. Kang have managed underbite cases across the full spectrum, from Phase 1 reverse-pull cases in elementary school children to combined surgical and orthodontic cases in adults.
Dr. Baharvand and Dr. Kang are a husband-and-wife orthodontic team based in Frisco, with three convenient locations serving families across Frisco, The Colony, Prosper, and Little Elm. Dr. Baharvand is ABO board-certified and a published clinician whose work has appeared in the American Journal of Orthodontics and Dentofacial Orthopedics.
1,000+
Five-star reviews across 3 locations
ABO
Board-certified orthodontist
Published
AJO-DO cover clinician
Free
Consultation with full diagnostic records
Our Locations
5605 FM 423, Suite 600
Frisco, TX 75036
FM 423 & Lebanon Rd — next to the UPS Store
4713 Highway 121, Suite 304
The Colony, TX 75056
FM 423 & Hwy 121 — next to Ross
2155 University Dr, Suite 110
Frisco, TX 75033
On 380 across from Cook Children’s Medical Center Prosper
Hours: Mon–Fri 8:00am–5:00pm | 972.538.4343
Suspect an Underbite? Don’t Wait. Get an Evaluation.
Free consultations at all three Elate Orthodontics locations include a complete diagnostic workup: digital scans, panoramic X-rays, clinical photos, and a clear explanation of whether your or your child’s underbite is skeletal, dental, or a combination. No pressure, no surprises, no commitment to treatment.
Also see: All Conditions We Treat | Overbite | All Treatments | Before & After | Meet Dr. B & Dr. Kang