Orthodontic Relapse Treatment in Frisco & The Colony, TX
Adult Retreatment by Dr. Baharvand & Dr. Kang — Identifying What Caused the Relapse, Plus Braces, Invisalign, Angel Aligners & Permanent Retention
📞 972.538.4343
Orthodontic relapse retreatment at Elate Orthodontics — finding what caused the shift, correcting it, and locking in the result
Orthodontic Relapse — Frisco & The Colony, TX
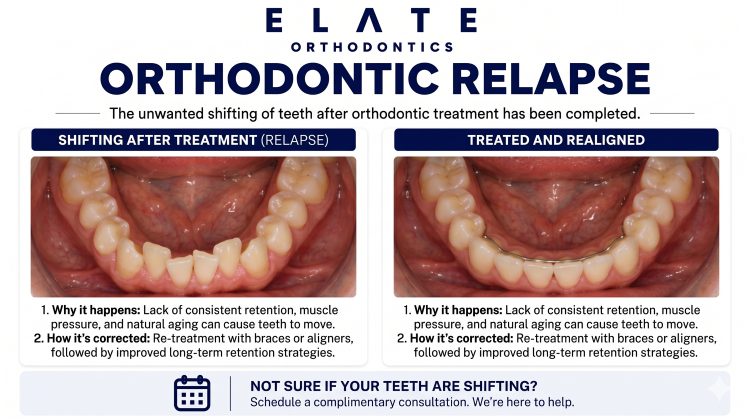
Teeth Move Throughout Life. The Real Question Is Why Your Teeth Shifted and How to Stop It From Happening Again.
Orthodontic relapse refers to teeth shifting back toward their pre-treatment positions after orthodontic treatment ended. Some degree of tooth movement throughout life is normal — teeth continue to drift in subtle ways into adulthood and beyond, regardless of whether someone had braces. What concerns most adults is more dramatic relapse: visible crowding returning, gaps reopening, the bite changing, or the smile no longer looking the way it did when treatment ended. The good news is that retreatment is highly effective. The more important news is that retreatment without addressing what caused the relapse usually produces another cycle of shifting. Successful retreatment requires identifying the underlying cause and correcting it, not just repositioning the teeth.
At Elate Orthodontics, Dr. Kevin Baharvand and Dr. Julia Kang see adult patients across Frisco, The Colony, Prosper, and Little Elm who had orthodontic treatment years ago and now have teeth that have shifted. Many were teenagers when they had braces. Some never wore retainers as instructed, others lost their retainers years ago, and many were never told that retention is a lifelong commitment. Some have undiagnosed tongue thrust or other habits that drove the relapse, while others simply experienced the natural drift that all teeth show over decades. Our approach is the same in every case: diagnose what caused the shift, plan retreatment that addresses both the alignment and the cause, and design retention that holds the result long-term.
As an ABO board-certified practice with a published clinician on staff, our diagnostic approach reflects the depth of training that distinguishes specialty orthodontic care. We take comprehensive records at every consultation and explain exactly what we see using your own digital scans, panoramic X-rays, and clinical photos. For relapse cases, we look for the underlying drivers that other practices sometimes miss and discuss honestly what retreatment can achieve and what is needed to maintain the result.
The Common Patterns of Orthodontic Relapse
Lower Front Tooth Crowding
The most common pattern of orthodontic relapse. The lower front teeth gradually rotate, overlap, and crowd over years after braces, even in patients who initially had a beautiful result. This pattern is so consistent that some clinicians consider it a near-universal feature of long-term post-orthodontic change. The physiology is partly natural drift and partly the influence of bite forces, tongue position, and lip pressure that continues for life.
For this pattern, retreatment with a permanent bonded retainer behind the lower front teeth is often the most effective long-term solution. The thin wire is invisible and dramatically reduces the chance of repeat relapse. See our crooked teeth page for more.
Reopening of Gaps
Gaps that were closed during orthodontic treatment commonly reopen years later, particularly midline gaps between the upper front teeth and gaps closed by extracting teeth. This pattern is frequently driven by undiagnosed tongue thrust pushing the front teeth apart with each swallow. Treatment that does not address the tongue habit usually produces another cycle of gap closure followed by gap reopening.
For these cases, retreatment combined with myofunctional therapy and permanent bonded retainers is the most reliable approach. See our gapped teeth page for more.
Bite & Open Bite Relapse
Some patients experience relapse of bite issues — the open bite returns, the overbite deepens, or the previously corrected crossbite redevelops. This pattern is most common when the original treatment did not address an underlying habit driver like tongue thrust, mouth breathing, or persistent thumb sucking. The bite issue and the cause work together, and treating only the bite alignment without correcting the cause often produces this kind of relapse.
Retreatment for these patterns typically requires combining orthodontic correction with myofunctional therapy or coordination with ENT specialists if airway issues are involved. See our open bite page for more.
Late Adult Drift Pattern
Some patients in their 30s, 40s, or 50s notice their teeth have shifted into mild crowding or rotation that was not present immediately after their braces came off. This pattern is partly the natural drift that all adults experience as the bone and ligaments around teeth gradually remodel over decades. It is not always indicative of a specific underlying cause and is one of the reasons retainer wear ideally continues lifelong, even years after orthodontic treatment ended.
For these cases, retreatment with clear aligners and permanent retention often produces excellent outcomes with minimal disruption to adult life.
Most patients have a combination of these patterns. Comprehensive evaluation identifies which factors drove the relapse and the right retreatment plan.
The Underlying Drivers
What Causes Orthodontic Relapse?
By far the most common cause of relapse. Many patients were never told that retention is a lifelong commitment, stopped wearing retainers within a year or two of treatment, lost their retainers years ago, or never received retainers that fit properly long-term. Without retention, teeth drift back toward their original positions over months to years. This is a problem the original treatment did not cause — it is a problem of how retention was managed afterward.
One of the most commonly missed contributors to relapse. The tongue applies pressure thousands of times per day during swallowing. When a patient has tongue thrust that pushes the tongue forward against the front teeth, that pressure gradually moves the front teeth forward, opens gaps, and reverses orthodontic results. Patients with relapse and a history of open bite, gaps, or flared front teeth often have undiagnosed tongue thrust as the underlying driver.
Patients with chronic mouth breathing have low tongue posture during the day and night, which removes the normal tongue support of the upper jaw. This contributes to crowding development and can drive bite changes that look like relapse but are actually ongoing skeletal and dental changes from the underlying airway issue. See our mouth breathing page for more.
Wisdom teeth pushing forward and crowding the front teeth is a popular theory but is more controversial than many patients realize. Modern research suggests wisdom teeth are often blamed for crowding that has other causes including natural drift, tongue habits, and inadequate retention. Some patients do experience crowding that coincides with wisdom tooth eruption. We discuss wisdom teeth honestly during evaluation rather than offering them as a simple explanation for all relapse cases.
Teeth and the bone supporting them continue to remodel slowly throughout life. Mild crowding and rotation can develop in the 30s, 40s, and beyond even in patients with good retainer wear and no underlying habits. This natural drift is one reason retention is increasingly recommended as a lifelong commitment rather than a temporary post-treatment phase.
In patients with gum disease and periodontal bone loss, teeth often drift more dramatically because the supporting structures are compromised. Front teeth can flare forward, gaps can open, and the bite can change as the periodontal foundation deteriorates. Addressing the periodontal disease in coordination with a periodontist is essential before orthodontic retreatment, otherwise retreatment results will not hold.
Why Addressing Relapse Matters
Most adult patients with orthodontic relapse come to us motivated by aesthetics — their smile no longer looks the way it did and they want it back. That is a completely valid reason to seek retreatment. There are also functional reasons that matter long-term. Crowded lower teeth are harder to clean and more prone to gum disease and decay. Reopened gaps can affect speech and eating function. Bite issues that have returned or worsened can contribute to uneven tooth wear, jaw stress, and TMJ-related discomfort over time. Addressing relapse before it progresses produces simpler treatment and better long-term outcomes.
More importantly, identifying and addressing the underlying cause — whether that is tongue thrust, mouth breathing, periodontal disease, or simply inadequate retention — is what determines whether retreatment results last. Treating the visible problem without addressing the cause typically produces another cycle of relapse within a few years.
What Untreated Relapse Causes
Progressive crowding that becomes more severe and harder to treat over time
Gaps that continue to widen as forward tongue pressure continues unchecked
Bite changes that produce uneven tooth wear and accelerated dental aging
Increased risk of gum disease and decay in crowded areas that are difficult to clean
Self-consciousness about a smile that no longer looks the way it should
More complex retreatment if relapse continues to progress over additional years
Frustration that the original investment in orthodontic treatment seems to have been undone
Treatment Approach
How We Approach Orthodontic Relapse Retreatment
Relapse retreatment is fundamentally an adult treatment category — most patients seeking retreatment had their original braces as teenagers and are now in their 20s, 30s, 40s, or beyond. Our approach is the same regardless of age: identify what caused the shift, plan retreatment that addresses both the alignment and the cause, and design retention that holds the result long-term.
Mild Relapse (Minor Shifting)
For mild lower front tooth crowding or minor reopening of small gaps, retreatment is often straightforward and relatively quick. Clear aligners typically work very well for these cases. Treatment time is often 4 to 8 months, sometimes shorter. The retention plan after retreatment is typically more important than the retreatment itself for ensuring the result lasts.
For most mild relapse cases, we strongly recommend a permanent bonded retainer in addition to a removable retainer to dramatically reduce the chance of further shifting.
Moderate Relapse
For moderate crowding, gap reopening, or bite changes, retreatment is typically more involved. Treatment time often runs 12 to 18 months with comprehensive orthodontics using clear aligners or braces. Identifying and addressing the underlying cause — particularly tongue thrust if present — is essential to prevent another cycle of relapse.
These cases benefit most from comprehensive diagnostic evaluation that looks beyond the visible alignment to find what drove the shift in the first place.
Significant Relapse with Bite Changes
For significant relapse where the bite has substantially changed — open bite returned, severe crowding redeveloped, jaw misalignment progressed — retreatment is comprehensive and often combines orthodontics with myofunctional therapy, periodontal coordination if gum issues are present, and other specialist input. Treatment time is typically 18 to 24 months.
These cases often involve adults whose original orthodontic treatment did not address the underlying cause, and who are now finding that retreatment with cause-focused care produces results that last.
Treatment Options
Treatments We Use for Orthodontic Relapse
Invisalign
Often the preferred option for adult relapse retreatment. Clear aligners work very well for mild to moderate crowding, gap closure, and most relapse patterns. Treatment is virtually invisible during the day and removable for eating and important events. Modern Invisalign protocols handle the great majority of relapse cases effectively. Comprehensive treatment typically takes 8 to 18 months depending on severity.
Angel Aligners
A clear aligner system we offer at Elate Orthodontics for appropriate cases. Like other clear aligner brands, Angel Aligners can correct most relapse patterns effectively when treatment is paired with cause-focused care and good retention afterward. We discuss whether Invisalign or Angel Aligners is a better fit for each patient based on case complexity and individual factors.
Clear Braces
For relapse cases requiring complex movements or where aligners would not produce predictable results, clear braces give us tooth-colored brackets with the precise mechanics of braces. A great option for adults who want braces-level predictability without the visibility of metal.
Traditional Braces
For severe relapse or complex bite changes that have redeveloped over years, traditional braces provide the most reliable mechanics for the most demanding cases. Used selectively when aligners would not be the right choice for the specific case.
Permanent Bonded Retainers
The single most important component of relapse retreatment. A small wire bonded behind the lower front teeth (and sometimes the upper) holds the teeth in their corrected positions full-time, dramatically reducing the chance of repeat relapse. Modern bonded retainers are durable, comfortable, and invisible from the front. We strongly recommend permanent retention for all relapse retreatment cases.
Removable Retainer Systems
Clear removable retainers worn nightly complement permanent bonded retainers for full-mouth retention. Together, the two systems provide redundant protection against future shifting. We design custom retention plans for each patient based on the relapse pattern, the underlying cause, and individual factors.
Myofunctional Therapy Coordination
For relapse cases where tongue thrust or other oral muscle patterns drove the original shift, myofunctional therapy is essential to prevent another cycle of relapse. We coordinate with myofunctional therapists in the Frisco area as part of comprehensive cause-focused retreatment.
Periodontist & Specialist Coordination
For relapse cases where periodontal disease, mouth breathing, or other underlying conditions are contributing, we coordinate with periodontists, ENT specialists, and other providers as needed. Addressing the broader picture is what produces retreatment results that last decades rather than years.
When to Address Relapse
Earlier Retreatment Is Almost Always Simpler Than Later Retreatment
Relapse tends to progress over years. The mild lower front tooth crowding noticed at age 28 often becomes more severe by age 40 if not addressed. The gap that reopened slightly at age 32 may have widened substantially by age 50. Addressing relapse when it is mild typically requires shorter, simpler treatment than addressing the same case after additional years of progression. The cause that drove the original relapse is also still active during those years and continues affecting the teeth.
Our approach to retreatment is direct: we tell you what we think caused the relapse, what retreatment can realistically achieve, what retention is needed to maintain the result long-term, and what additional care from other specialists may be helpful. The combination of cause-focused diagnosis, well-designed retreatment, and lifelong retention is what produces results that last.
See Real Outcomes
Relapse Retreatment Cases From Our Practice
Our before-and-after gallery includes real adult retreatment cases at Elate Orthodontics, ranging from mild lower front tooth crowding addressed in months with clear aligners, to comprehensive cases combining retreatment with myofunctional therapy and permanent retention, to complex cases involving periodontal coordination and full-mouth restoration. Each case shows the diagnosis, the cause-focused approach, and the final result.
Common Questions
Orthodontic Relapse FAQ
This is the most common question we get from adult patients. The most likely causes are inadequate retention (retainers were not worn long-term or were lost), undiagnosed tongue thrust pushing teeth forward over years, natural drift that affects all teeth throughout life, or a combination of these factors. Identifying which cause is dominant in your specific case guides the right retreatment approach. We diagnose this directly during evaluation rather than assuming a single explanation.
Yes, in the great majority of relapse cases. Invisalign is often our preferred option for adult retreatment because it works very well for the typical relapse patterns (mild to moderate crowding, gap closure, minor bite issues), is virtually invisible during treatment, and requires fewer office visits than braces. Treatment time is typically 8 to 18 months depending on severity. We discuss whether Invisalign is the best option for your specific case during consultation.
Treatment time depends on severity. Mild relapse cases (minor lower front tooth crowding, small gap reopening) often take 4 to 8 months. Moderate cases typically take 12 to 18 months. Significant cases with bite changes typically take 18 to 24 months. Most adult retreatment is shorter than original orthodontic treatment because the teeth have already been moved into approximately correct positions previously.
Without addressing the underlying cause and committing to lifelong retention, yes — the same factors that caused the original relapse will continue working. With cause-focused retreatment (addressing tongue thrust, mouth breathing, periodontal disease, or other drivers when present) and permanent bonded retainers, the chance of significant repeat relapse is dramatically reduced. We design retention plans that protect the retreatment investment.
Wisdom teeth as the cause of crowding is more controversial than many patients realize. Modern research suggests wisdom teeth are often blamed for crowding that has other causes, including natural drift and tongue habits. Some patients do have relapse that coincides with wisdom tooth eruption, while others develop the same crowding even after wisdom teeth are removed. We evaluate this honestly during your consultation rather than offering wisdom teeth as a simple explanation.
Coverage for orthodontic retreatment varies significantly by plan. Some PPO dental insurance plans cover orthodontics once per lifetime regardless of whether the patient had treatment as a child, while others have specific exclusions for retreatment. We help patients understand what their plan covers and offer flexible financing through Cherry to make retreatment accessible regardless of insurance coverage.
Why Frisco & The Colony Adults Choose Elate Orthodontics for Relapse Retreatment
Orthodontic relapse retreatment is one of the categories where the difference between practices that look beyond the visible problem and practices that just realign the teeth matters most. Many adult patients have been through retreatment elsewhere only to find their teeth shifting again because the underlying cause was never identified. The willingness to look for tongue thrust, the discipline to coordinate with myofunctional therapists when needed, and the commitment to designing retention that holds long-term are what separate good outcomes from great ones. Dr. Baharvand and Dr. Kang screen for these factors during every adult retreatment evaluation.
Dr. Baharvand and Dr. Kang are a husband-and-wife orthodontic team based in Frisco, with three convenient locations serving families across Frisco, The Colony, Prosper, and Little Elm. Dr. Baharvand is ABO board-certified and a published clinician whose work has appeared in the American Journal of Orthodontics and Dentofacial Orthopedics.
1,000+
Five-star reviews across 3 locations
ABO
Board-certified orthodontist
Published
AJO-DO cover clinician
Free
Consultation with full diagnostic records
Our Locations
5605 FM 423, Suite 600
Frisco, TX 75036
FM 423 & Lebanon Rd — next to the UPS Store
4713 Highway 121, Suite 304
The Colony, TX 75056
FM 423 & Hwy 121 — next to Ross
2155 University Dr, Suite 110
Frisco, TX 75033
On 380 across from Cook Children’s Medical Center Prosper
Hours: Mon–Fri 8:00am–5:00pm | 972.538.4343
Teeth Shifting Back? Let’s Find Out Why and Make It Last This Time.
Free consultations at all three Elate Orthodontics locations include a complete diagnostic workup: digital scans, panoramic X-rays, clinical photos, and screening for the underlying causes that may have driven your relapse. We design retreatment that addresses both the alignment and the cause, with retention that holds the result long-term. No pressure, no surprises, no commitment to treatment.
Also see: All Conditions We Treat | Crooked Teeth | Gapped Teeth | Tongue Thrust | Retainers | Before & After