Protruding Teeth Treatment in Frisco & The Colony, TX
Buck Teeth & Front Tooth Protrusion — Treated by Dr. Baharvand & Dr. Kang with Braces, Invisalign, Angel Aligners & Growth Modification
📞 972.538.4343
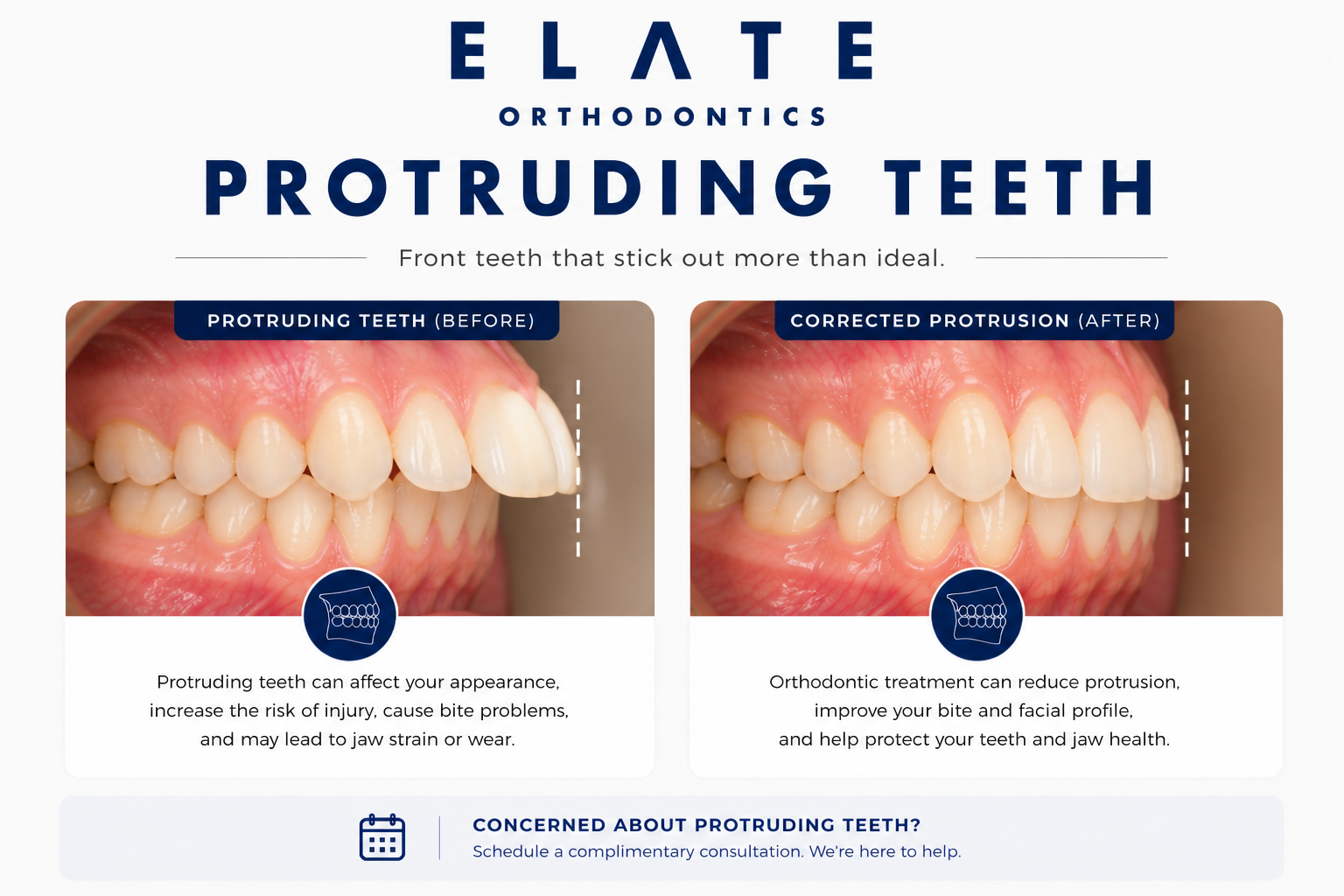
Protruding teeth correction at Elate Orthodontics — protecting front teeth from injury and restoring confidence
Protruding Teeth — Frisco & The Colony, TX
Protruding Front Teeth Are More Than a Cosmetic Concern — They’re a Real Injury Risk
Protruding teeth, sometimes called “buck teeth” or excessive overjet, are upper front teeth that angle outward or sit far ahead of the lower teeth. The clinical measurement is called overjet — the horizontal distance between the upper and lower front teeth when biting down. A normal overjet is around 2 millimeters. Anything significantly larger means the upper teeth are protruding, either because they are tipped forward, because the lower jaw has not grown forward enough, or both. Protruding teeth are most often a sign of a Class II skeletal pattern.
At Elate Orthodontics, Dr. Kevin Baharvand and Dr. Julia Kang treat protruding teeth in patients across Frisco, The Colony, Prosper, and Little Elm. We tell parents this directly: protruding teeth in children are not just a cosmetic issue. Children with significant overjet are at much higher risk of dental trauma if they fall, are hit in the mouth during sports, or are involved in any kind of accident. Protruding upper teeth are simply more exposed and more vulnerable. This is one of the conditions where early evaluation and treatment can prevent permanent damage.
As an ABO board-certified practice with a published clinician on staff, our diagnostic approach reflects the depth of training that distinguishes specialty orthodontic care. We take comprehensive records at every consultation and explain exactly what we see using your own digital scans, panoramic X-rays, and clinical photos. For protruding teeth, we identify whether the protrusion is dental (tipped teeth on healthy jaws) or skeletal (jaw size mismatch) because the treatment approach differs significantly.
Skeletal vs. Dental Protrusion (And Why the Difference Matters)
Skeletal Protrusion (Class II Pattern)
Skeletal protrusion means the jaws themselves are mismatched in size or position. The most common pattern is a small or recessed lower jaw that has not grown forward enough to meet the upper jaw. The upper teeth may sit in normal positions on the upper jaw, but they look protruded because the lower jaw is set back. This is what most people picture when they think of “buck teeth.” It is genetic and runs in families.
Skeletal protrusion in growing children responds well to growth modification appliances that encourage the lower jaw to develop forward. Catching it during active growth can dramatically reduce treatment complexity and often eliminates the need for jaw surgery later.
Dental Protrusion (Tipped Teeth)
Dental protrusion means the jaws are well-positioned, but the upper front teeth themselves are tipped or angled forward. The skeletal foundation is normal. The teeth simply lean outward. This often results from prolonged thumb sucking, tongue thrust, or arch crowding that pushes front teeth outward.
Dental protrusion is usually simpler to correct with braces or clear aligners and does not require growth modification or surgery. The contributing habit (thumb sucking, tongue thrust) usually needs to be addressed alongside treatment to prevent relapse.
Diagnosing whether protrusion is skeletal, dental, or a combination determines the entire treatment plan. This is why a specialist’s diagnosis matters — particularly for growing children where treatment timing affects what’s possible.
Underlying Causes
What Causes Protruding Teeth?
The most common cause of significant protrusion is a lower jaw that has not grown forward enough during development. The upper teeth may be in normal positions on the upper jaw, but the relative position of the lower jaw makes them appear protruded. This is genetic and is typically addressed during active growth using functional appliances that encourage the lower jaw to develop forward.
Persistent thumb sucking or pacifier use past age 4 to 5 directly pushes the upper front teeth forward. The thumb or pacifier acts as a wedge between the front teeth, tipping them outward over years of constant pressure. Stopping the habit is the first step. Once the habit has stopped, the structural changes typically need orthodontic correction.
When the tongue pushes forward against the front teeth during swallowing or at rest, it can flare the upper front teeth outward over time. Thousands of swallows per day add up, and tongue thrust is one of the most common reasons protrusion relapses after correction. We screen for tongue posture during evaluation and frequently coordinate with myofunctional therapists when needed.
Like other malocclusions, protrusion has a strong genetic component. Jaw size, jaw position, and growth direction are largely inherited. If one or both parents had protruding teeth or required orthodontic treatment for buck teeth, their children are at higher likelihood of developing similar patterns. We often see siblings with similar profiles.
When there is not enough room in the dental arch for all the teeth, the front teeth often flare forward as a release valve. The front teeth are pushed outward by pressure from the back teeth that have nowhere else to go. Treatment typically involves creating space and then retracting the front teeth to a healthier position.
When children chronically mouth-breathe or have difficulty closing their lips comfortably over the front teeth (called lip incompetence), the muscle balance that normally keeps front teeth in proper position is disrupted. Without lip pressure restraining the teeth, they tend to flare outward. Addressing the airway component is often part of the treatment plan.
The Real Risk: Dental Trauma in Children
The most important thing parents should understand about protruding teeth in children is the elevated injury risk. Multiple studies have shown that children with overjet greater than 3 millimeters are about twice as likely to suffer dental trauma to the upper front teeth compared to children with normal overjet. Children with overjet greater than 6 millimeters have an even higher risk. The math is simple: protruding teeth are more exposed and have less protection from the upper lip during falls or impacts.
Permanent front teeth that are fractured, knocked out, or damaged in childhood often need lifelong restorative care including root canals, crowns, or eventual implants. Reducing protrusion before adolescence — through Phase 1 treatment when appropriate — meaningfully lowers this risk and is one of the strongest reasons for early evaluation.
What Untreated Protrusion Causes
Significantly higher risk of dental trauma to the upper front teeth in children and teens
Permanent damage to front teeth from sports, falls, or accidents (often requiring lifelong restorative care)
Difficulty closing lips comfortably over the front teeth, leading to dry mouth and gum problems
Speech difficulties, particularly with sounds requiring tongue contact with front teeth
Self-consciousness and social impact, particularly during the school years and adolescence
Bite issues from the mismatch between upper and lower teeth, accelerating wear patterns
Loss of the non-surgical correction window for skeletal cases as growth completes in late adolescence
Treatment Approach
How We Treat Protruding Teeth at Every Age
Protrusion treatment depends heavily on age and on whether the underlying cause is skeletal or dental. Treatment options expand significantly during childhood and adolescence because the jaws are still growing. Adult treatment is excellent but works through different mechanics. The right approach is determined by comprehensive diagnosis at the consultation.
Children (Ages 7–10)
For young children with significant protrusion, particularly cases with skeletal Class II patterns, Phase 1 treatment can be powerful. Functional appliances encourage the lower jaw to grow forward during the active growth window. Early intervention also reduces dental trauma risk during the school years and often shortens or simplifies later orthodontic treatment.
Not every child with protruding teeth needs Phase 1. We monitor and recommend treatment when the timing and clinical picture genuinely benefit from intervention.
Teens (Ages 11–17)
The teen years are the prime treatment window for most protrusion cases. Comprehensive treatment with braces or clear aligners — often combined with elastics that bring the lower jaw forward and the upper teeth back — produces excellent outcomes. For skeletal cases, growth modification can still be effective during the pubertal growth spurt.
For teens with severe skeletal protrusion where camouflage will not produce a stable result, treatment may be planned alongside future orthognathic surgery in late adolescence.
Adults
In adults, growth modification is no longer an option since the jaws are fully developed. Dental protrusion in adults is highly treatable with braces or clear aligners, sometimes with selective extractions to create space for retracting the front teeth. Mild to moderate skeletal protrusion can be camouflaged orthodontically with strategic tooth movement.
For adults with severe skeletal protrusion where camouflage will not produce a stable result, we coordinate with experienced oral surgeons for jaw surgery combined with orthodontic treatment. We tell you honestly which path is realistic for your case.
Treatment Options
Treatments We Use to Correct Protruding Teeth
Traditional Braces
The most versatile option for moderate to severe protrusion. Braces give us precise control to retract the front teeth and work seamlessly with elastics that bring the lower jaw forward and the upper teeth back. The gold standard for cases combining protrusion with bite correction.
Clear Braces
Same effective mechanics as traditional braces with tooth-colored brackets. A great option for teens and adults treating protrusion who want the predictability of braces with less visibility during treatment.
Invisalign
Modern Invisalign protocols with precision attachments and Class II elastics handle the majority of protrusion cases — particularly mild to moderate dental protrusion in cooperative patients. Invisalign Teen also addresses growing patients with combined growth modification approaches.
Angel Aligners
A clear aligner system we offer at Elate Orthodontics for appropriate cases. Like other clear aligner brands, Angel Aligners can correct mild to moderate dental protrusion with precision attachments and elastic-driven mechanics tailored to each patient’s anatomy.
Growth Modification (Phase 1)
For growing children and teens with skeletal Class II protrusion, functional appliances encourage the lower jaw to develop forward during active growth. Caught at the right age, growth modification can dramatically reduce protrusion, lower dental trauma risk, and often eliminate the need for jaw surgery later.
Habit Appliances & Myofunctional Therapy
For protrusion driven by thumb sucking or tongue thrust, habit appliances help children stop the contributing behavior. Myofunctional therapy retrains tongue posture and swallowing patterns. Without addressing these underlying habits, protrusion often relapses after orthodontic correction.
Selective Extractions
For severe dental protrusion in adults — particularly cases with significant crowding — selective extraction of premolars creates space to retract the front teeth into healthier positions. Extraction therapy is reserved for cases where it is genuinely needed and produces the best long-term outcome. We discuss this honestly when it applies.
Orthognathic Surgery (Severe Adult Cases)
For adults with severe skeletal protrusion where orthodontic treatment alone cannot produce a stable, healthy bite, we coordinate with experienced oral surgeons for jaw surgery combined with orthodontic treatment. Reserved for cases that genuinely require it.
AAO Recommendation
Early Evaluation Reduces Injury Risk and Expands Treatment Options
The American Association of Orthodontists recommends an evaluation by age 7. For protruding teeth, this matters for two reasons. First, children with significant overjet are at meaningfully higher risk of dental trauma during the school and middle school years, and Phase 1 treatment can reduce that risk before injuries happen. Second, skeletal protrusion responds best to growth modification during active growth — the same case caught at age 25 may require jaw surgery instead.
If your child has visibly protruding upper teeth, especially if they cannot close their lips comfortably over them, schedule an evaluation. Most children evaluated at age 7 do not need treatment yet. The point is to identify which children should be monitored, which will benefit from Phase 1, and which can wait until adolescence.
See Real Outcomes
Protruding Teeth Cases From Our Practice
Our before-and-after gallery includes real protrusion corrections at Elate Orthodontics, ranging from Phase 1 cases in growing children corrected with functional appliances to comprehensive teen and adult cases corrected with braces, clear aligners, or surgical coordination. Each case shows the diagnosis, the appliances used, and the final result.
Common Questions
Protruding Teeth FAQ
Yes — “buck teeth” is the everyday term for protruding upper front teeth, which clinicians call excessive overjet. Both terms describe the same condition: upper front teeth that angle outward or sit far ahead of the lower teeth. The clinical measurement is overjet, which is the horizontal distance between upper and lower front teeth when biting down.
Yes, particularly in children and teens. Multiple studies have shown that children with overjet greater than 3 millimeters are about twice as likely to suffer dental trauma compared to children with normal overjet. Children with overjet greater than 6 millimeters have an even higher risk. Reducing protrusion through Phase 1 treatment when appropriate is one of the strongest reasons for early orthodontic care.
Yes, for mild to moderate dental protrusion in cooperative patients. Modern Invisalign protocols include precision attachments and Class II elastics that effectively retract the front teeth and improve overjet. For severe skeletal protrusion or cases requiring significant growth modification, traditional braces combined with functional appliances often produce more predictable results.
Some mild dental protrusion in young children improves naturally as the bite settles in and the lower jaw catches up to the upper jaw during growth. Significant skeletal protrusion typically does not improve on its own and often worsens during adolescence as the upper jaw outgrows the lower jaw further. The only way to know which category your child falls into is an orthodontic evaluation. The age 7 evaluation is designed for exactly this.
Phase 1 treatment for skeletal protrusion in young children typically takes 9 to 14 months. Comprehensive teen and adult treatment generally takes 18 to 24 months. Adult cases involving extractions or surgical coordination may take longer. We give you a realistic timeline at consultation based on your specific case.
Most PPO dental insurance plans include orthodontic benefits that apply to protruding teeth treatment, particularly when there is documented functional concern such as elevated trauma risk or lip incompetence. Coverage varies by plan. We are in-network with most major PPO carriers and offer flexible financing through Cherry to make treatment accessible regardless of insurance coverage.
Why Frisco & The Colony Families Choose Elate Orthodontics for Protruding Teeth
Protruding teeth treatment is one of the strongest cases for early orthodontic evaluation. The depth of the diagnosis (skeletal vs. dental), the experience to time growth modification correctly, and the willingness to address contributing factors like thumb sucking or tongue thrust are what separate good outcomes from great ones. Dr. Baharvand and Dr. Kang have managed protrusion cases across the full spectrum, from Phase 1 functional appliance treatment in elementary school children to complex adult cases combining alignment with surgical coordination.
Dr. Baharvand and Dr. Kang are a husband-and-wife orthodontic team based in Frisco, with three convenient locations serving families across Frisco, The Colony, Prosper, and Little Elm. Dr. Baharvand is ABO board-certified and a published clinician whose work has appeared in the American Journal of Orthodontics and Dentofacial Orthopedics.
1,000+
Five-star reviews across 3 locations
ABO
Board-certified orthodontist
Published
AJO-DO cover clinician
Free
Consultation with full diagnostic records
Our Locations
5605 FM 423, Suite 600
Frisco, TX 75036
FM 423 & Lebanon Rd — next to the UPS Store
4713 Highway 121, Suite 304
The Colony, TX 75056
FM 423 & Hwy 121 — next to Ross
2155 University Dr, Suite 110
Frisco, TX 75033
On 380 across from Cook Children’s Medical Center Prosper
Hours: Mon–Fri 8:00am–5:00pm | 972.538.4343
Concerned About Protruding Teeth? Don’t Wait — Especially for Kids.
Free consultations at all three Elate Orthodontics locations include a complete diagnostic workup: digital scans, panoramic X-rays, clinical photos, and a clear explanation of whether the protrusion is skeletal, dental, or a combination. We design treatment that protects your child’s front teeth and produces lasting results. No pressure, no surprises, no commitment to treatment.
Also see: All Conditions We Treat | Overbite | Underbite | Crooked Teeth | Gapped Teeth | Before & After