Ectopic Eruption Treatment in Frisco & The Colony, TX
Catching Wrong-Path Eruption Early — Treated by Dr. Baharvand & Dr. Kang with Phase 1 Intervention, Braces, Invisalign & Angel Aligners
📞 972.538.4343
Ectopic eruption correction at Elate Orthodontics — redirecting wrong-path teeth before they become impacted
Ectopic Eruption — Frisco & The Colony, TX
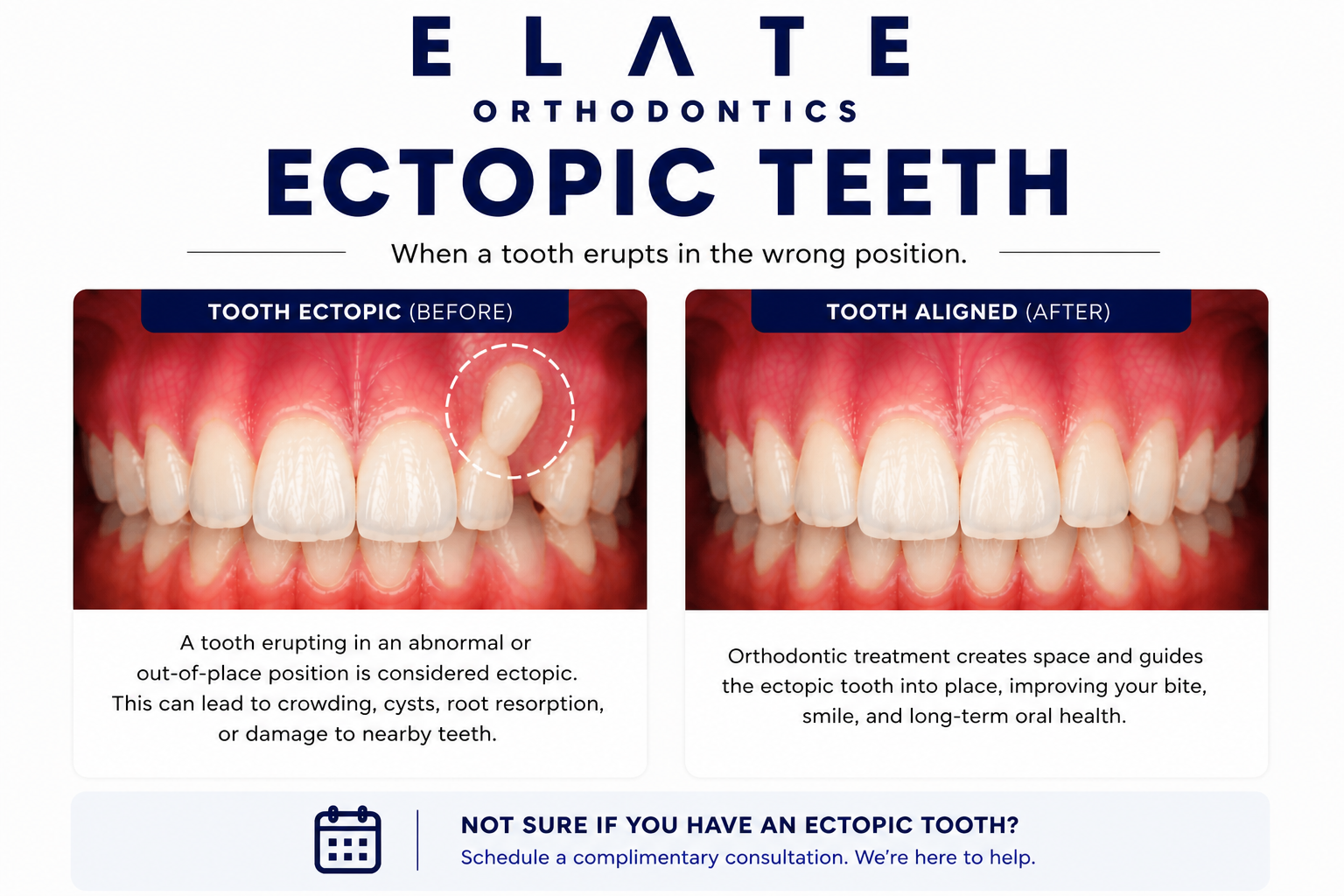
When a Tooth Erupts in the Wrong Position, Catching It Early Often Avoids Impaction
Ectopic eruption refers to a tooth that erupts (or attempts to erupt) into an abnormal position rather than its proper place in the dental arch. Most often, ectopic eruption is identified during late childhood — between ages 6 and 12 — when permanent teeth are coming in. The most common patterns are first permanent molars erupting forward and getting caught under the back of the second baby molar, upper canines drifting toward the lateral incisor instead of erupting straight down, and lateral incisors erupting behind the front teeth instead of next to them.
At Elate Orthodontics, Dr. Kevin Baharvand and Dr. Julia Kang treat ectopic eruption in patients across Frisco, The Colony, Prosper, and Little Elm. Ectopic eruption is essentially the early warning sign for impaction. A tooth heading in the wrong direction at age 8 to 10 has time to be redirected with relatively simple intervention. The same tooth left alone often becomes fully impacted by adolescence and requires surgical exposure with orthodontic traction. Catching ectopic eruption early is one of the strongest practical reasons for the AAO age-7 evaluation, and it is one of the most rewarding categories of pediatric orthodontic care because the difference between early and late intervention is so dramatic.
As an ABO board-certified practice with a published clinician on staff, our diagnostic approach reflects the depth of training that distinguishes specialty orthodontic care. We take comprehensive records at every consultation including panoramic X-rays, which allow us to see developing permanent teeth still inside the bone and identify ectopic eruption patterns long before they become visible problems. For at-risk children, we monitor over time and intervene at exactly the right moment.
The Most Common Ectopic Eruption Patterns
Ectopic First Permanent Molars
The single most common form of ectopic eruption. The upper first permanent molar attempts to erupt around age 6, and instead of coming in vertically, it tips forward and gets caught under the back of the second primary molar (the second baby tooth in the back). The molar essentially gets stuck and cannot fully erupt. If left alone, the second baby molar often loses its root from the pressure and falls out prematurely, while the permanent molar remains tipped forward.
Caught early, ectopic first molars are highly correctable with simple appliances that tip the molar back into proper position. The intervention is typically much simpler than impaction treatment and prevents space loss that would lead to crowding later.
Ectopic Canine Eruption
Upper canines have the longest eruption path of any tooth and are particularly prone to drifting in the wrong direction. Ectopic canine eruption typically becomes visible on a panoramic X-ray between ages 9 and 12 — the canine appears to be heading toward the lateral incisor (or even the central incisor) rather than coming straight down into its proper position next to the lateral incisor. This is the early warning sign for canine impaction.
Caught at this stage, simple interventions like removing the baby canine and addressing crowding with palatal expansion can sometimes redirect the permanent canine into its proper position. Caught after the canine is fully impacted in adolescence, treatment requires surgical exposure and 12 to 18 months of orthodontic traction.
Ectopic Lateral Incisors
When a permanent lateral incisor (the tooth next to the front teeth) erupts behind the front teeth instead of next to them, this is called lingual eruption or ectopic lateral. It is most often caused by insufficient space in the arch or a baby tooth that did not fall out on time. Parents often notice the lateral coming in behind the existing baby tooth before that baby tooth has fallen out.
Treatment depends on the severity. Mild cases sometimes self-correct as the patient continues to grow and the baby tooth falls out. More significant cases benefit from removal of the lingering baby tooth and orthodontic guidance to bring the lateral into proper position before the bone forms around it in the wrong place.
Other Ectopic Eruption Patterns
Less common ectopic patterns include central incisors blocked from erupting by supernumerary teeth (extra teeth in the bone), second permanent molars erupting with a forward tilt similar to first molars, and lower second premolars drifting from their proper positions when their primary tooth predecessor is lost too early. Each pattern has its own treatment timing and approach.
For all ectopic eruption cases, the principle is the same: the earlier the diagnosis, the simpler and more predictable the intervention. We use panoramic X-rays at every comprehensive evaluation to identify these patterns before they become advanced.
Ectopic eruption is essentially the early stage of impaction. Catching it before the tooth becomes truly stuck is the difference between simple intervention and complex surgical-orthodontic recovery.
Underlying Causes
What Causes Ectopic Eruption?
The most common cause of ectopic eruption is simply not enough room. When the arch is too narrow or too short to accommodate the developing permanent teeth, they often deflect from their normal eruption path and end up in the wrong position. Crowding identified early can sometimes be addressed with palatal expansion to create the room developing teeth need.
When a baby tooth does not fall out on schedule, it can deflect the developing permanent tooth from its normal eruption path. This is one of the most common causes of ectopic lateral incisor eruption. The permanent tooth, blocked by the persistent baby tooth, finds an alternative path and often comes in behind or to the side of where it should be.
Eruption patterns have a strong genetic component. If a parent or sibling had ectopic eruption — particularly canine impaction or ectopic first molars — the patient is at higher risk of similar patterns. Family history is one of our routine evaluation questions for children in the eruption window, and it changes how closely we monitor.
Some children develop extra teeth in the bone that should not be there. These supernumerary teeth can physically block the eruption path of permanent teeth, particularly in the front of the mouth where a small extra tooth (called a mesiodens) commonly forms between the upper central incisors. Removal of the supernumerary tooth typically allows normal eruption to resume.
Childhood injuries — particularly to the front teeth during the toddler years — can disrupt the developing permanent tooth bud underneath. These early traumas are often forgotten by the time the permanent tooth attempts to erupt several years later, but they can cause the permanent tooth to develop in an unusual position or with abnormal direction of eruption.
When a baby tooth is lost too early — usually due to severe decay or injury — neighboring teeth can drift into the empty space, blocking the future eruption path of the permanent successor. This is particularly common with early loss of baby molars, which often leads to ectopic eruption of premolars years later. Space maintainers prevent this drift when used appropriately.
Why Catching Ectopic Eruption Early Matters So Much
Ectopic eruption is one of the conditions where the difference between early and late intervention is most dramatic. A first permanent molar caught at age 7 with simple intervention typically takes a few months to redirect with a simple appliance. The same molar left alone often causes premature loss of the second baby molar, space loss in the arch, and crowding that leads to extractions years later.
Similarly, an ectopic canine identified on X-ray at age 10 can sometimes be redirected with simple interventions. Left alone, that same canine often becomes fully impacted by age 15, requiring surgical exposure and 12 to 18 months of orthodontic traction. The mathematics of early intervention almost always favor catching ectopic eruption early.
What Untreated Ectopic Eruption Causes
Progression to full impaction, requiring complex surgical-orthodontic recovery instead of simple intervention
Premature loss of baby teeth from pressure of permanent teeth in wrong positions
Space loss in the arch as neighboring teeth drift into the gap left by ectopic eruption
Damage to the roots of adjacent teeth from pressure of an ectopic permanent tooth, particularly with ectopic canines
Crowding that often leads to extractions in adolescence when it could have been prevented with timely intervention
More complex and longer treatment when ectopic eruption is allowed to progress to impaction
Loss of the simple-intervention window once teeth become fully impacted in adolescence
Treatment Approach
How We Treat Ectopic Eruption
Ectopic eruption is fundamentally a pediatric condition — it is identified and treated during childhood and early adolescence when permanent teeth are erupting. The treatment depends on which tooth is affected and how far along the ectopic pattern has progressed.
Children (Ages 6–10) — The Prime Window
This is the prime treatment window for most ectopic eruption cases. Ectopic first permanent molars are typically identified between ages 6 and 8 and corrected with simple appliances. Ectopic eruption of incisors is usually addressed by removing lingering baby teeth and guiding the permanent tooth into position. Early signs of ectopic canine eruption can be intercepted before the canine becomes fully impacted.
Most children with mild ectopic patterns do not need treatment yet. We monitor over time and intervene at exactly the right moment.
Teens (Ages 11–17)
By the teen years, ectopic eruption that was not caught earlier has often progressed to full impaction. Treatment shifts from simple Phase 1 intervention to comprehensive orthodontics combined with surgical exposure and orthodontic traction. The principles are similar but the execution is more involved and treatment time is longer.
For teens with ectopic eruption that did not become fully impacted, comprehensive treatment with braces or aligners can still bring teeth into proper position, particularly when space is available and the tooth has not become ankylosed.
Adults
In adults, ectopic eruption presents as legacy issues — teeth that erupted years ago in unusual positions and remained there. Treatment uses comprehensive orthodontics to align these teeth properly, sometimes combined with selective extractions or restorative coordination depending on the position. Adult cases can produce excellent results, though they take longer than catching the same pattern in childhood.
For adults whose ectopic eruption progressed to full impaction during adolescence and was not addressed, the treatment approach mirrors what is described on our tooth impaction page.
Treatment Options
Treatments We Use to Correct Ectopic Eruption
Phase 1 Interceptive Treatment
The defining treatment for ectopic eruption in growing children. Simple appliances designed to redirect the eruption path of permanent teeth before they become fully impacted. Highly effective when caught in the right window and dramatically simpler than treating impaction in adolescence.
Selective Baby Tooth Removal
For ectopic eruption caused by lingering baby teeth or where removing a baby tooth will redirect the permanent tooth into proper position, we coordinate with pediatric dentists for timely extraction. The most common application is removing a baby canine to redirect an ectopic permanent canine, which can sometimes prevent canine impaction entirely.
Palatal Expander
For ectopic eruption driven by insufficient arch space, palatal expansion creates the physical room developing teeth need to find their proper positions. Particularly effective for ectopic canines and ectopic incisors when caught early during the active growth window.
Space Maintainers & Space Regainers
Small appliances that hold or recover space lost when a baby tooth has fallen out too early or when an ectopic first molar has caused space loss. Space management at this age can dramatically simplify or eliminate the need for later orthodontic treatment.
Traditional Braces
For comprehensive treatment that includes correcting ectopic eruption alongside other issues, braces give us precise control over each tooth and remain the most reliable option for cases requiring complex movements. Often used in adolescence when ectopic patterns were not caught earlier.
Clear Braces
Same effective mechanics as traditional braces with tooth-colored brackets. A great option for teens and adults treating legacy ectopic eruption issues who want the predictability of braces with less visibility during treatment.
Invisalign
Modern Invisalign protocols handle most adolescent and adult cases involving legacy ectopic eruption issues with excellent outcomes. Particularly effective when the ectopic tooth is fully erupted but in the wrong position, requiring repositioning rather than recovery from impaction.
Angel Aligners
A clear aligner system we offer at Elate Orthodontics for appropriate cases. Like other clear aligner brands, Angel Aligners can correct ectopic eruption issues in cases where the teeth have erupted but require repositioning, with treatment plans tailored to each patient’s anatomy.
Surgical Coordination
For cases where ectopic eruption is being blocked by supernumerary teeth, cysts, or other obstacles in the bone, we coordinate with oral surgeons for removal of the obstruction. Once the path is clear, normal eruption often resumes or orthodontic guidance can bring the tooth into position.
AAO Recommendation
Ectopic Eruption Is Why the Age-7 Evaluation Exists
The American Association of Orthodontists recommends an evaluation by age 7. Ectopic eruption is one of the strongest practical reasons for this recommendation. By age 7, the first permanent molars and front teeth are typically erupting, panoramic X-rays can show developing canines and premolars still inside the bone, and we can identify ectopic eruption patterns before they cause damage. Catching ectopic first molars at age 6 to 8 typically requires a simple appliance worn for a few months. Catching the same case at age 12 often requires comprehensive orthodontic treatment.
Most children evaluated at age 7 do not need treatment yet. The point of the evaluation is to identify the small percentage of children with ectopic eruption patterns or other developmental issues where early intervention will prevent much larger problems. We monitor at no charge between the age-7 visit and the appropriate treatment timing for each child.
See Real Outcomes
Ectopic Eruption Cases From Our Practice
Our before-and-after gallery includes real ectopic eruption cases at Elate Orthodontics, ranging from Phase 1 corrections of ectopic first molars in young children, to early canine redirection that prevented full impaction, to comprehensive teen and adult cases addressing legacy ectopic eruption issues. Each case shows the diagnosis, the appliances used, and the final result.
Common Questions
Ectopic Eruption FAQ
Ectopic eruption is the early stage when a tooth is heading in the wrong direction or attempting to erupt in an abnormal position. Impaction is the later stage when the tooth has become fully stuck and cannot erupt on its own. Ectopic eruption left untreated often progresses to impaction. Catching it at the ectopic stage is dramatically simpler than treating it after impaction has occurred.
This is a fairly common pattern, particularly with lower front teeth, and is usually called shark teeth by parents. In many cases the baby tooth falls out on its own and the permanent tooth drifts forward into proper position over a few months. If the baby tooth does not fall out within several weeks or the permanent tooth is significantly out of position, an orthodontic evaluation is warranted to determine if intervention is needed.
A panoramic X-ray taken during the age 7 to 12 window shows developing permanent teeth still inside the bone alongside the teeth that have already erupted. From this image, we can see the eruption path of canines, premolars, and second molars and identify when one is heading in the wrong direction long before it becomes a visible problem. This is why early radiographic evaluation matters even when the smile looks fine to parents.
Not necessarily. Many ectopic eruption cases are managed with simple Phase 1 interventions that do not involve full braces. A child treated for an ectopic first molar at age 7 may not need any further orthodontic treatment beyond that initial correction. Other children may benefit from comprehensive orthodontic treatment in adolescence after Phase 1 has resolved the immediate issue. We give you a realistic outlook based on each individual case.
Phase 1 treatment for ectopic first molars typically takes 3 to 9 months. Treatment for ectopic incisors usually takes 6 to 12 months depending on severity. Early canine redirection through baby tooth removal and palatal expansion typically takes 9 to 14 months and is followed by monitoring. Comprehensive treatment in adolescence for legacy ectopic issues typically takes 18 to 24 months.
Most PPO dental insurance plans include orthodontic benefits that apply to ectopic eruption treatment, particularly Phase 1 interceptive treatment in young children. Coverage varies by plan, with some plans covering Phase 1 separately from comprehensive treatment in adolescence. We are in-network with most major PPO carriers and offer flexible financing through Cherry to make treatment accessible regardless of insurance coverage.
Why Frisco & The Colony Families Choose Elate Orthodontics for Ectopic Eruption
Ectopic eruption is one of the most rewarding categories of pediatric orthodontic care because the difference between early and late intervention is so dramatic. The depth of the diagnosis, the experience to interpret panoramic X-rays correctly, and the discipline to monitor at no charge between the age-7 evaluation and the appropriate treatment timing are what separate good outcomes from great ones. Dr. Baharvand and Dr. Kang have managed thousands of ectopic eruption cases across the full spectrum, from simple Phase 1 first molar corrections to complex multi-tooth eruption disturbance cases.
Dr. Baharvand and Dr. Kang are a husband-and-wife orthodontic team based in Frisco, with three convenient locations serving families across Frisco, The Colony, Prosper, and Little Elm. Dr. Baharvand is ABO board-certified and a published clinician whose work has appeared in the American Journal of Orthodontics and Dentofacial Orthopedics.
1,000+
Five-star reviews across 3 locations
ABO
Board-certified orthodontist
Published
AJO-DO cover clinician
Free
Consultation with full diagnostic records
Our Locations
5605 FM 423, Suite 600
Frisco, TX 75036
FM 423 & Lebanon Rd — next to the UPS Store
4713 Highway 121, Suite 304
The Colony, TX 75056
FM 423 & Hwy 121 — next to Ross
2155 University Dr, Suite 110
Frisco, TX 75033
On 380 across from Cook Children’s Medical Center Prosper
Hours: Mon–Fri 8:00am–5:00pm | 972.538.4343
Tooth Coming In Wrong? Let’s Catch It Before It Becomes Impacted.
Free consultations at all three Elate Orthodontics locations include a complete diagnostic workup: digital scans, panoramic X-rays, clinical photos, and identification of any ectopic eruption patterns developing in your child’s mouth. We monitor at no charge between evaluations and intervene at exactly the right moment. No pressure, no surprises, no commitment to treatment.
Also see: All Conditions We Treat | Tooth Impaction | Crowded Teeth | Pediatric Orthodontics | Before & After